

Effects of exenatide alone and in combination with daclizumab on beta-cell function in long-standing type 1 diabetes
- PMID: 19808924
- PMCID: PMC2782986
- DOI: 10.2337/dc09-0773
Effects of exenatide alone and in combination with daclizumab on beta-cell function in long-standing type 1 diabetes
Abstract
Objective: In patients with long-standing type 1 diabetes, we investigated whether improved beta-cell function can be achieved by combining intensive insulin therapy with agents that may 1) promote beta-cell growth and/or limit beta-cell apoptosis and 2) weaken the anti-beta-cell autoimmunity.
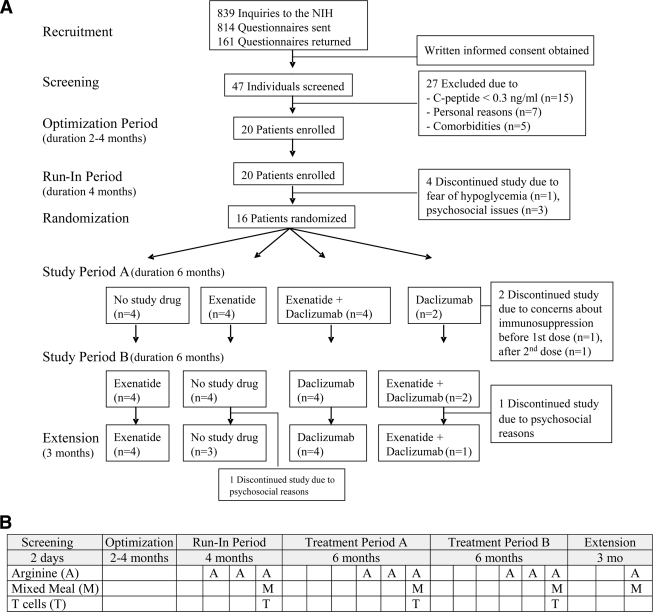
Research design and methods: For this study, 20 individuals (mean age 39.5 +/- 11.1 years) with long-standing type 1 diabetes (21.3 +/- 10.7 years) were enrolled in this prospective open-label crossover trial. After achieving optimal blood glucose control, 16 subjects were randomized to exenatide with or without daclizumab. Endogenous insulin production was determined by repeatedly measuring serum C-peptide.
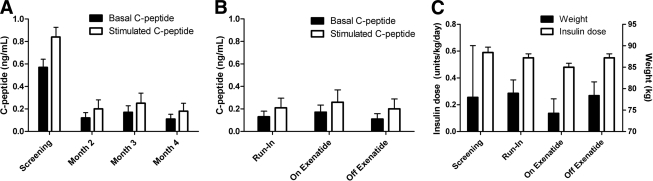
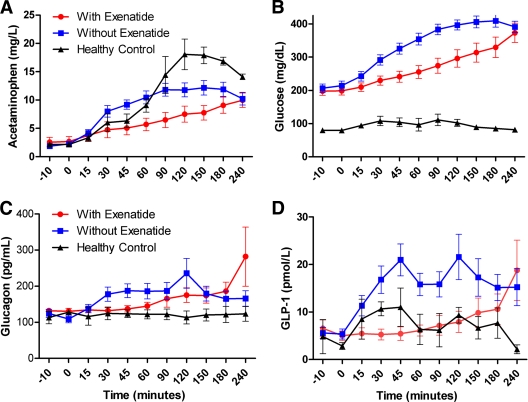
Results: In 85% of individuals with long-standing type 1 diabetes who were screened for participation in this trial, C-peptide levels >or=0.05 ng/ml (0.02 nmol/l) were found. Residual beta-cells responded to physiological (mixed-meal) and pharmacological (arginine) stimuli. During exenatide treatment, patients lost 4.1 +/- 2.9 kg body wt and insulin requirements declined significantly (total daily dose on exenatide 0.48 +/- 0.11 vs. 0.55 +/- 0.13 units x kg(-1) x day(-1) without exenatide; P = 0.0062). No signs of further activation of the underlying autoimmune disease were observed. Exenatide delayed gastric emptying, suppressed endogenous incretin levels, but did not increase C-peptide secretion.
Conclusions: In long-standing type 1 diabetes, which remains an active autoimmune disease even decades after its onset, surviving beta-cells secrete insulin in a physiologically regulated manner. However, the combination of intensified insulin therapy, exenatide, and daclizumab did not induce improved function of these remaining beta-cells.
Trial registration: ClinicalTrials.gov NCT00064714.
Figures
References
-
- Hirshberg B, Rother KI, Digon BJ, 3rd, Lee J, Gaglia JL, Hines K, Read EJ, Chang R, Wood BJ, Harlan DM: Benefits and risks of solitary islet transplantation for type 1 diabetes using steroid-sparing immunosuppression: the National Institutes of Health experience. Diabetes Care 2003; 26: 3288– 3295 - PubMed
-
- Dor Y, Brown J, Martinez OI, Melton DA: Adult pancreatic beta-cells are formed by self-duplication rather than stem-cell differentiation. Nature 2004; 429: 41– 46 - PubMed
-
- Teta M, Rankin MM, Long SY, Stein GM, Kushner JA: Growth and regeneration of adult beta cells does not involve specialized progenitors. Dev Cell 2007; 12: 817– 826 - PubMed
-
- Herold KC, Gitelman SE, Masharani U, Hagopian W, Bisikirska B, Donaldson D, Rother K, Diamond B, Harlan DM, Bluestone JA: A single course of anti-CD3 monoclonal antibody hOKT3γ1(Ala-Ala) results in improvement in C-peptide responses and clinical parameters for at least 2 years after onset of type 1 diabetes. Diabetes 2005; 54: 1763– 1769 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
