

Emerging infections in burns
- PMID: 19810827
- PMCID: PMC2956561
- DOI: 10.1089/sur.2009.024
Emerging infections in burns
Abstract
Background: Patients who suffer severe burns are at higher risk for local and systemic infections. In recent years, emerging resistant pathogens have forced burn care providers world wide to search for alternative forms of treatment. Multidrug-resistant Staphylococcus aureus, Pseudomonas aeruginosa, Acinetobacter spp., and various fungal strains have been the major contributors to the increase in morbidity and mortality rates. Multi-drug-resistant S. aureus remains the major cause of gram-positive burn wound infections world wide. Treatment strategies include rigorous isolation protocols and new types of antibiotics where necessary.
Methods: We reviewed 398 severely burned patients (burns >40% total body surface area [TBSA]) admitted to our hospital between 2000 and 2006. Patients who did not contract multi-drug-resistant gram-negative organisms during their hospital course and received our standard antibiotic regimen-vancomycin and piperacillin/tazobactam-served as controls (piperacillin/tazobactam; n = 280). The treatment group consisted of patients who, during their acute hospital stay, developed infections with multi-drug-resistant gram-negative pathogens and were treated with vancomycin and colistin for at least three days (colistin; n = 118).
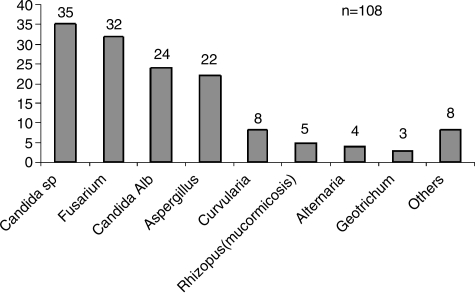
Results: Gram-negative organisms continue to cause the most severe infections in burn patients. Colistin has re-emerged as a highly effective antibiotic against multiresistant Pseudomonas and Acinetobacter infections of burns. Patients who required colistin therapy had a significantly larger average total and full-thickness burn than patients treated with piperacillin/tazobactam and vancomycin, and the mortality rate was significantly higher in the colistin group (p < 0.05). However, there was no significant difference between the colistin and piperacillin/tazobactam groups in the incidence of neurotoxicity, hepatic toxicity, or nephrotoxicity. The main fungal pathogens in burn patients are Candida spp., Aspergillus spp., and Fusarium spp. A definitive diagnosis is more difficult to obtain than in bacterial infections. Amphotericin B and voriconazole remain the two most important anti-fungal substances in our practice.
Conclusions: Innovations in fluid management, ventilatory support, surgical care, and antimicrobial therapy have contributed to a significant reduction in morbidity and mortality rates in burn patients. Vancomycin and clindamycin are the two most important reserve antibiotics for methicillin-resistant Staphylococcus aureus infection. Oxazolidinones and streptogramins have showed high effectiveness against gram-positive infections. Colistin has re-emerged as a highly effective antibiotic against multiresistant Pseudomonas and Acinetobacter infections. Current challenges include Candida, Aspergillus, and molds. The development of new agents, prudent and appropriate use of antibiotics, and better infection control protocols are paramount in the ongoing battle against multi-resistant organisms.
Figures
References
-
- Herndon DN. Barrow RE. History of treatments of burns. In: Herndon DN, editor. Total Burn Care. 3rd. Philadelphia: WB Saunders; 2007. pp. 1–8.
-
- Muller MJ. Herndon DN. The challenge of burns. Lancet. 1994;343:216–220. - PubMed
-
- Saffle JR. Davis B. Williams P. Recent outcomes in the treatment of burn injury in the United States: A report from the American Burn Association Patient Registry. J Burn Care Rehabil. 1995;16:219–232. - PubMed
-
- Baxter CR. Shires T. Physiological response to crystalloid resuscitation of severe burns. Ann NY Acad Sci. 1968;150:874–894. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
