

Hypertension, systemic inflammation and body weight in relation to lung function impairment-an epidemiological study
- PMID: 19811383
- PMCID: PMC3334274
- DOI: 10.1080/15412550903049157
Hypertension, systemic inflammation and body weight in relation to lung function impairment-an epidemiological study
Abstract
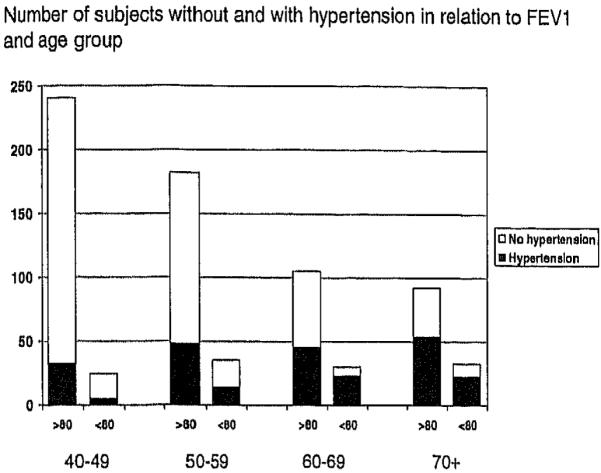
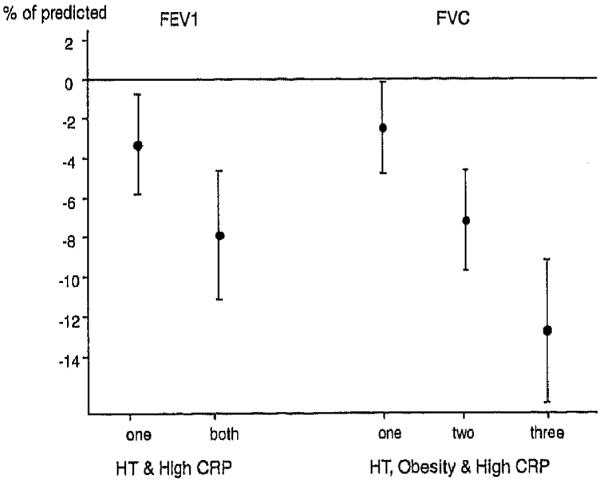
Recent reports on the simultaneous occurrence of systemic inflammation and airflow obstruction are usually based on a highly selective patient population, but their importance warrants further evaluation in the general population. The objectives were to study the interrelationship between airflow obstruction, smoking, hypertension, obesity and CRP as a marker of systemic inflammation in a randomly selected sample of the general Icelandic population (n = 939). This study comprised 758 randomly selected men and women 40 years and older living in Reykjavik, Iceland, and who were participating in the Burden of Obstructive Lung Disease (BOLD) study (81% response rate). In addition to the BOLD protocol, which included post-bronchodilator spirometry, they answered questions about general health and medication. Serum samples were taken for measurement of C-reactive protein (CRP). In the sample-245 individuals (33%) reported having hypertension. Subjects with hypertension were older, had a higher BMI and higher CRP levels. Subjects with hypertension had lower values of FEV(1) than predicted (89.9 +/- 18.5 vs. 94.5 +/- 14.4%) (p < 0.001) and FVC (92.2 +/- 15.1 vs. 95.3 +/- 12.3%) (p = 0.002). These differences remained significant after adjusting for age, BMI, CRP and smoking. Hypertension and CRP levels above the median were both independently and additively associated with lower FEV(1) and FVC. In addition a lower FVC% was also associated with a higher BMI (> 30 mg/m2). Use of betablocking antihypertensives was not related to lung function. Hypertension, BMI and systemic inflammation affect lung function independently of each other. All three variables have a negative effect on FVC, while hypertension and high CRP were independently associated with impaired FEV(1).
Figures
References
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS, GOLD Scientific Committee Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256–1276. - PubMed
-
- Mannino DM, Buist AS. Global burden of COPD: Risk factory prevalence, and future trends. Lancet. 2007 Sep 1;370(9589):765–773. Review. - PubMed
-
- Rutten FH, Cramer MJ, Lammers JW, Grobbee DE, Hoes AW. Heart failure and chronic obstructive pulmonary disease: An ignored combination? Eur J Heart Fail. 2006 Nov;8(7):706–711. Review. - PubMed
-
- Rana JS, Mittleman MA, Sheikh J, Hu FB, Manson JE, Coldltz GA, Speizer FE, Barr RG, Camargo CA., Jr. Chronic obstructive pulmonary disease, asthma, and risk of type 2 diabetes in women. Diabetes Care. 2004 Oct;27(10):2478–2484. - PubMed
-
- Jørgensen NR, Schwarz P. Osteoporosis in chronic obstructive pulmonary disease patients. Curr Opin Pulm Med. 2008 Mar;14(2):122–127. Review. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous