

Impact of prematurity and co-morbidities on feeding milestones in neonates: a retrospective study
- PMID: 19812589
- PMCID: PMC2829105
- DOI: 10.1038/jp.2009.149
Impact of prematurity and co-morbidities on feeding milestones in neonates: a retrospective study
Abstract
Objective: Feeding problems are an important area of neonatal morbidity that requires attention. We defined the feeding milestones related to transition to per oral feeding among premature infants based on gestational (GA) and postmenstrual ages (PMA), and elucidated the co-morbidity variables affecting with these skills.
Study design: Feeding progress was tracked during the first hospitalization in a retrospective study involving 186 infants. We measured the age at acquisition of first feedings, maximum gavage feedings and maximum oral feedings. Resource usage measures included the total length of hospital stay (LOS), duration of gavage tube and duration of respiratory support. Effects of perinatal and co-morbidity factors on the acquisition of feeding milestones were evaluated. ANOVA, t-test, Wilcoxon rank sum test, chi(2) test, univariate and multivariate analysis, stepwise linear regression analysis and logistic regression analysis were applied as appropriate. Data were presented as mean+/-s.d., or as stated. P<0.05 was considered significant.
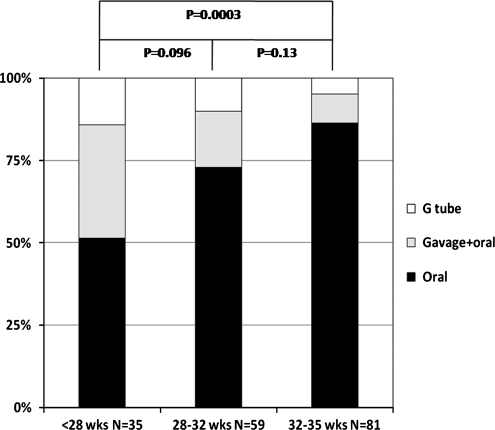
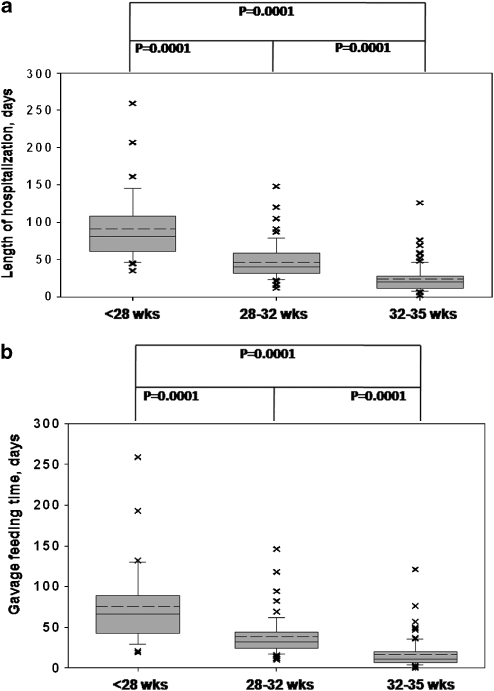
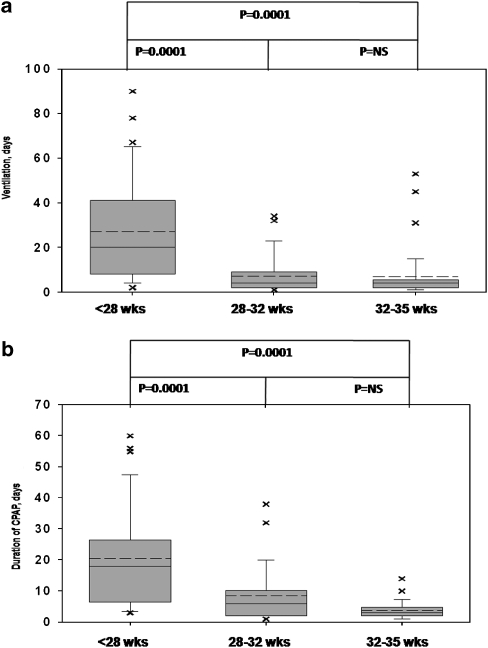
Result: We stratified the data into three groups based on GA at birth: <28.0 weeks (group-1), 28.0 to 32.0 weeks (group-2) and 32.0 to 35.0 weeks (group-3). Compared with group-3, group-1 needed four-fold more ventilation and five-fold more continuous positive airway pressure (CPAP) duration (all P<0.001); whereas group-2 needed two-fold more CPAP duration. Age at first feed correlated with age at full gavage feedings and age at full oral feedings (r=0.53 and r=0.71, both P<0.0001). Age at full gavage feedings correlated with age at full oral feedings (r=0.81, P<0.0001). Univariate analysis was significant for GA age, hypotension, the effects of gastroesophageal reflux, and duration of ventilation and CPAP on the PMA at maximal oral feedings (all P<0.05); multivariate analysis for these variables was also significant (R (2)=0.58, P<0.0001). The success rate for oral feedings at discharge accelerated with GA maturation and caffeine use; on the other hand, the need for respiratory support and management of positive blood culture were associated with failure rates (P<0.05).
Conclusion: Infants < 28 weeks GA have significant feeding delays with respect to initiation and progression to maximal gavage and oral feedings, as well as prolonged LOS. Infants >28 weeks GA attained successful feeding milestones by similar PMA. Specific aero-digestive co-morbidities significantly affected maximal oral feeding milestone. Delays in achieving maximum gavage and maximum oral feeding milestones suggest delays with the development of control and regulation of foregut motility.
Figures
References
-
- American Academy of Pediatrics, Committee on Children with Disabilities Managed care and children with special health care needs. Pediatrics. 2004;114:1693–1698. - PubMed
-
- American Academy of Pediatrics, Committee on Fetus and Newborn Hospital discharge of the high risk neonate: proposed guidelines. Pediatrics. 2008;122:1119–1126. - PubMed
-
- Hack M, Cartar L.Growth outcomes of preterm and very low birth weight infantsIn: Thureen PJ, Hay WW (eds). Neonatal Nutrition and Metabolism2nd ednCambridge University Press: Cambridge, UK; 2006640–653.
-
- Sadler TW.Special embryology: respiratory system and digestive systemIn: Sadler TW (ed). Langman's Medical Embryology7th ednWilliams and Wilkins: Baltimore, MD; 1995232–271.
