

Incidence of pregnancy after expectant, medical, or surgical management of spontaneous first trimester miscarriage: long term follow-up of miscarriage treatment (MIST) randomised controlled trial
- PMID: 19815581
- PMCID: PMC2759436
- DOI: 10.1136/bmj.b3827
Incidence of pregnancy after expectant, medical, or surgical management of spontaneous first trimester miscarriage: long term follow-up of miscarriage treatment (MIST) randomised controlled trial
Abstract
Objectives: To compare fertility rates after the three methods of managing early miscarriage in women recruited to the MIST (miscarriage treatment) randomised controlled trial.
Setting: Early pregnancy clinics of acute hospitals in the south west region of England.
Participants: 1199 women who had had an early miscarriage (<13 weeks) confirmed by scan.
Intervention: Expectant, medical, or surgical management.
Main outcome measures: Self reported pregnancy rates and live birth rates.
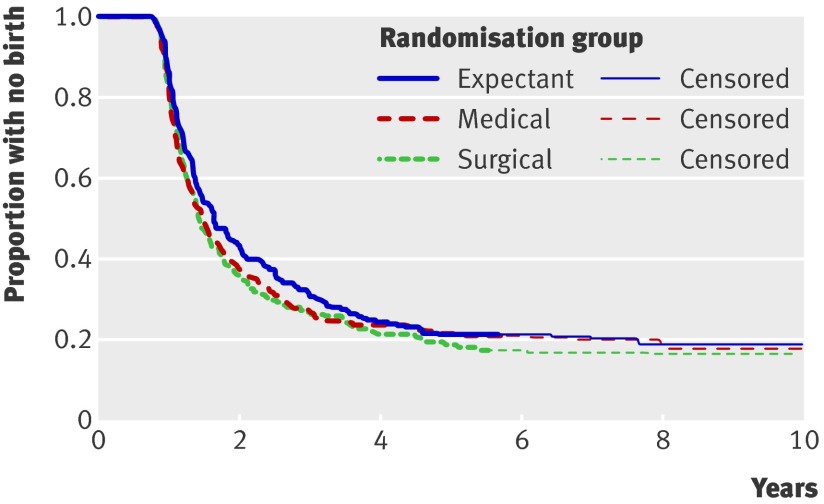
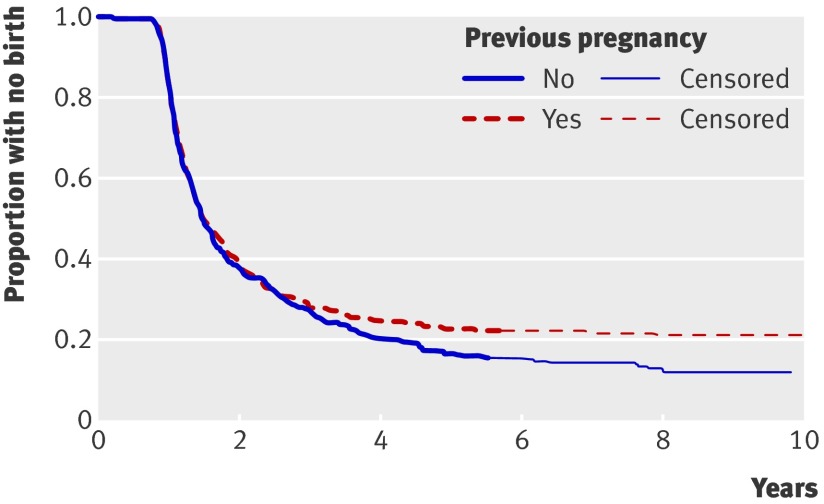
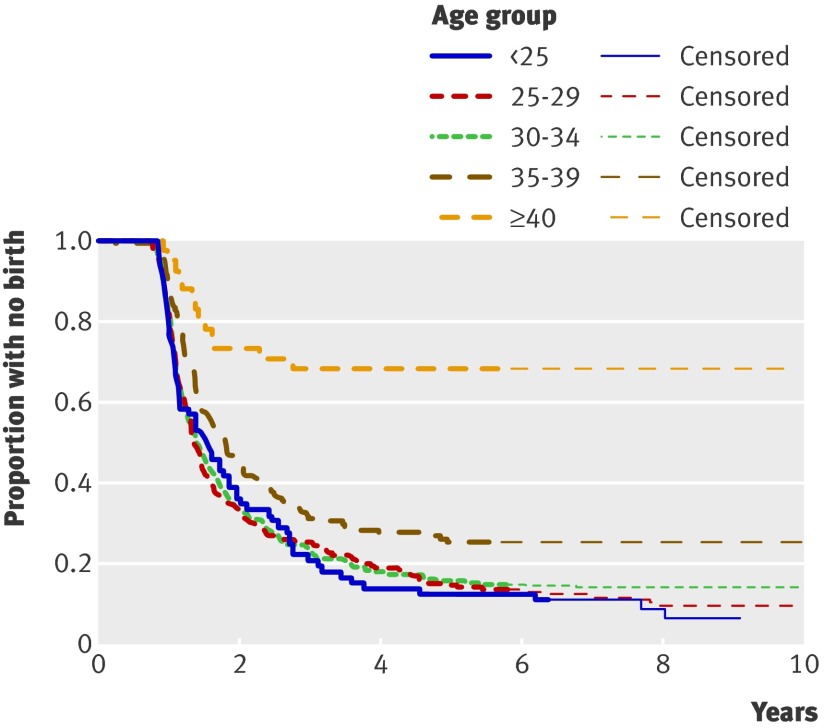
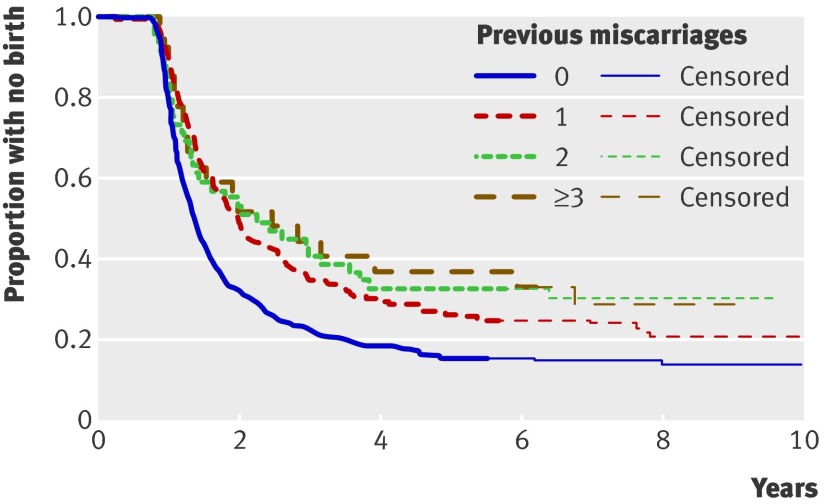
Results: Of 1199 women recruited to the trial, 1128 consented to follow-up. Of these, 762 women replied giving pregnancy details (68% response rate). Respondents were representative of the trial participants. The live birth rate five years after the index miscarriage was similar in the three management groups: 177/224 (79%, 95% confidence interval 73% to 84%) in the expectant management group, 181/230 (79%, 73% to 84%) in the medical group, and 192/235 (82%, 76% to 86%) in the surgical group. There was also no significant difference according to previous birth history. Older women and those with previous miscarriages were significantly less likely to subsequently give birth.
Conclusion: Method of miscarriage management does not affect subsequent pregnancy rates with around four in five women giving birth within five years of the index miscarriage. Women can be reassured that long term fertility concerns need not affect their choice of miscarriage management.
Trial registration: National Research Register N0467011677/N0467073587.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Clayton SG. Gynaecology by ten teachers. Edward Arnold, 1989.
-
- Ankum WM, Van der Veen F. Management of first-trimester spontaneous abortion. Lancet 1995;345:1179. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical