

Rituximab treatment of patients with severe, corticosteroid-resistant thyroid-associated ophthalmopathy
- PMID: 19818507
- PMCID: PMC2814962
- DOI: 10.1016/j.ophtha.2009.05.029
Rituximab treatment of patients with severe, corticosteroid-resistant thyroid-associated ophthalmopathy
Abstract
Purpose: To study the effectiveness of anti-CD20 (rituximab [RTX]; Rituxan; Genentech, Inc., South San Francisco, CA) therapy in patients with severe, corticosteroid (CS)-resistant thyroid-associated ophthalmopathy (TAO).
Design: Retrospective, interventional case series.
Participants: Six consecutive subjects with severe, progressive TAO unresponsive to CS.
Methods: Electronic medical record review of consecutive patients receiving RTX during the previous 18 months. Responses to therapy were graded using standard clinical assessment and flow cytometric analysis of peripheral lymphocytes.
Main outcome measures: Clinical activity score (CAS), proptosis, strabismus, treatment side effects, and quantification of regulatory T cells.
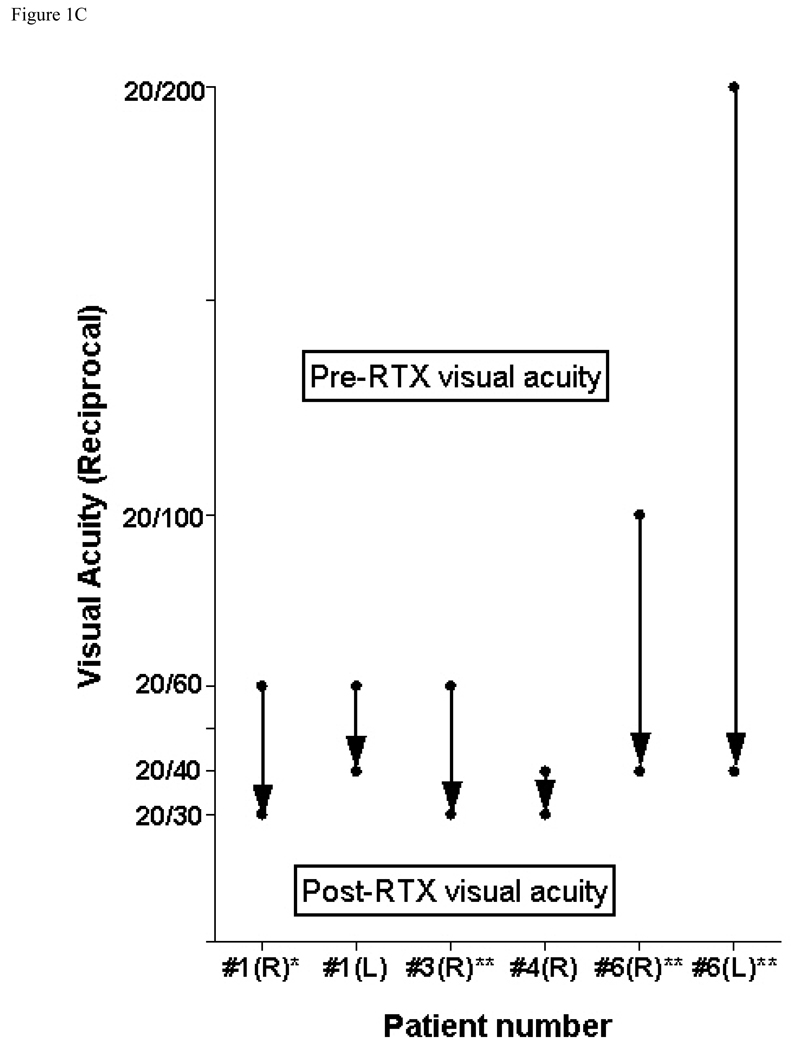
Results: Six patients were studied. Systemic CS failed to alter clinical activity in all patients (mean CAS+/-standard deviation, 5.3+/-1.0 before vs. 5.5+/-0.8 during therapy for 7.5+/-6.4 months; P = 1.0). However, after RTX treatment, CAS improved from 5.5+/-0.8 to 1.3+/-0.5 at 2 months after treatment (P<0.03) and remained quiescent in all patients (CAS, 0.7+/-0.8; P<0.0001) at a mean follow-up of 6.2+/-4.5 months. Vision improved bilaterally in all 4 patients with dysthyroid optic neuropathy (DON). None of the 6 patients experienced disease relapse after RTX infusion, and proptosis remained stable (Hertel measurement, 24+/-3.7 mm before therapy and 23.6+/-3.7 mm after therapy; P = 0.17). The abundance of T regulatory cells, assessed in 1 patient, increased within 1 week of RTX and remained elevated at 18 months of follow-up.
Conclusions: In progressive, CS-resistant TAO, rapid and sustained resolution of orbital inflammation and DON followed treatment with RTX.
Financial disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussed in this article.
Copyright 2010 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures






Comment in
-
Thyroid-associated orbitopathy.Ophthalmology. 2010 Sep;117(9):1864; author reply 1864-5. doi: 10.1016/j.ophtha.2010.05.006. Ophthalmology. 2010. PMID: 20816259 No abstract available.
-
Rituximab for thyroid eye disease.Ophthalmology. 2011 Apr;118(4):792; author reply 792-3. doi: 10.1016/j.ophtha.2011.01.012. Ophthalmology. 2011. PMID: 21459230 No abstract available.
References
-
- Jacobson DL, Gange SJ, Rose NR, Graham NM. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin Immunol Immunopathol. 1997;84:223–243. - PubMed
-
- McGrogan A, Seaman HE, Wright JW, de Vries CS. The incidence of autoimmune thyroid disease: a systematic review of the literature. Clin Endocrin (Oxf) 2008;69:687–696. - PubMed
-
- Weetman AP. Graves' disease. N Engl J Med. 2000;343:1236–1248. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
