

High lung allocation score is associated with increased morbidity and mortality following transplantation
- PMID: 19820072
- PMCID: PMC2832864
- DOI: 10.1378/chest.09-0319
High lung allocation score is associated with increased morbidity and mortality following transplantation
Abstract
Background: The lung allocation score (LAS) was initiated in May 2005 to allocate lungs based on medical urgency and posttransplant survival. The purpose of this study was to determine if there is an association between an elevated LAS at the time of transplantation and increased postoperative morbidity and mortality.
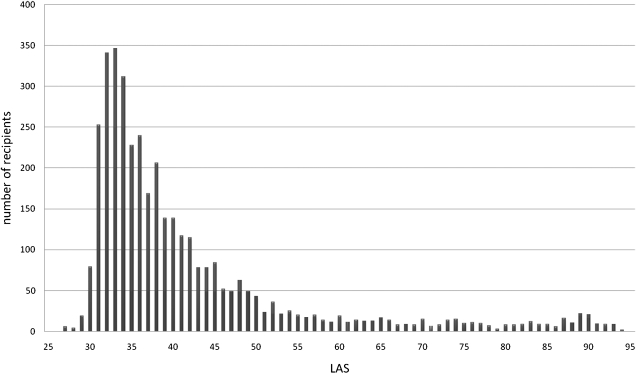
Methods: The United Network for Organ Sharing provided de-identified patient-level data. Analysis included lung transplant recipients aged >or= 12 years who received transplants between April 5, 2006, and December 31, 2007 (n = 3,836). Recipients were stratified into three groups: LAS < 50 (n = 3,161, 83.87%), LAS 50 to 75 (n = 411, 10.9%), and LAS >or= 75 (n = 197, 5.23%), referred to as low LAS (LLAS), intermediate LAS (ILAS), and high LAS (HLAS), respectively. The primary outcome was posttransplant graft survival at 1 year. Secondary outcomes included length of stay and in-hospital complications.
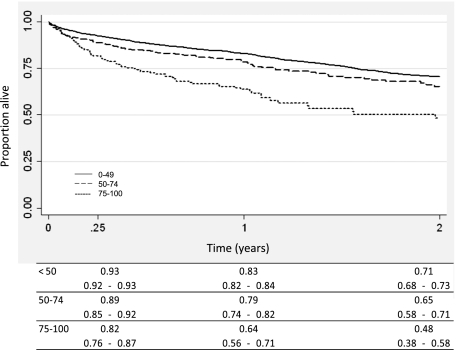
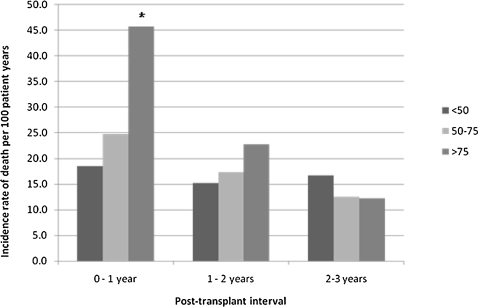
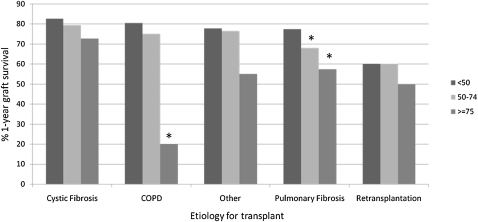
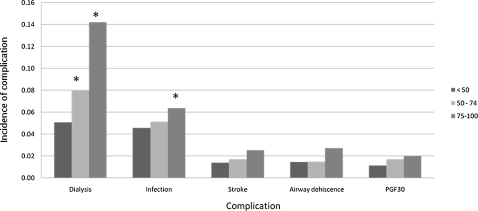
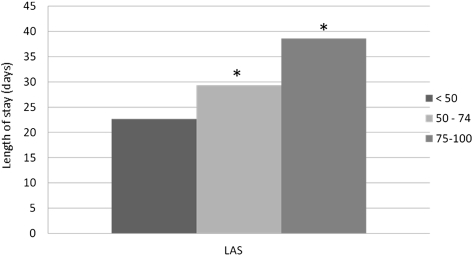
Results: HLAS recipients had significantly worse actuarial survival at 90 days and 1 year compared with LLAS recipients. When transplant recipients were stratified by disease etiology, a trend of decreased survival with elevated LAS was observed across all major causes of lung transplant. HLAS recipients were more likely to require dialysis or to have infections compared with LLAS recipients (P < .001). In addition, length of stay was higher in the HLAS group when compared with the LLAS group (P < .001).
Conclusions: HLAS is associated with decreased survival and increased complications during the transplant hospitalization. Whereas the LAS has improved organ allocation through decreased waiting list deaths and waiting list times, lower survival and higher morbidity among HLAS recipients suggests that continued review of LAS scoring is needed to ensure optimal long-term transplant survival.
Figures
References
-
- Levine GN, McCullough KP, Rodgers AM, Dickinson DM, Ashby VB, Schaubel DE. Analytical methods and database design: implications for transplant researchers, 2005. Am J Transplant. 2006;6(5 Pt 2):1228–1242. - PubMed
-
- Travaline JM, Cordova FC, Furukawa S, Criner GJ. Discrepancy between severity of lung impairment and seniority on the lung transplantation list. Transplant Proc. 2004;36(10):3156–3160. - PubMed
-
- The American Society for Transplant Physicians (ASTP)/American Thoracic Society(ATS)/European Respiratory Society(ERS)/International Society for Heart and Lung Transplantation(ISHLT) International guidelines for the selection of lung transplant candidates. Am J Respir Crit Care Med. 1998;158(1):335–339. - PubMed
-
- Egan TM, Kotloff RM. Pro/con debate: lung allocation should be based on medical urgency and transplant survival and not on waiting time. Chest. 2005;128(1):407–415. - PubMed
-
- De Meester J, Smits JM, Persijn GG, Haverich A. Listing for lung transplantation: life expectancy and transplant effect, stratified by type of end-stage lung disease, the Eurotransplant experience. J Heart Lung Transplant. 2001;20(5):518–524. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
