

Conventional occlusion versus pharmacologic penalization for amblyopia
- PMID: 19821369
- PMCID: PMC3804306
- DOI: 10.1002/14651858.CD006460.pub2
Conventional occlusion versus pharmacologic penalization for amblyopia
Update in
-
Conventional occlusion versus pharmacologic penalization for amblyopia.Cochrane Database Syst Rev. 2019 Aug 28;8(8):CD006460. doi: 10.1002/14651858.CD006460.pub3. Cochrane Database Syst Rev. 2019. PMID: 31461545 Free PMC article.
Abstract
Background: Amblyopia is defined as defective visual acuity in one or both eyes without demonstrable abnormality of the visual pathway, and is not immediately resolved by wearing glasses.
Objectives: To assess the effectiveness and safety of conventional occlusion versus atropine penalization for amblyopia.
Search strategy: We searched CENTRAL, MEDLINE, EMBASE, LILACS, the WHO International Clinical Trials Registry Platform, preference lists, science citation index and ongoing trials up to June 2009.
Selection criteria: We included randomized/quasi-randomized controlled trials comparing conventional occlusion to atropine penalization for amblyopia.
Data collection and analysis: Two authors independently screened abstracts and full text articles, abstracted data, and assessed the risk of bias.
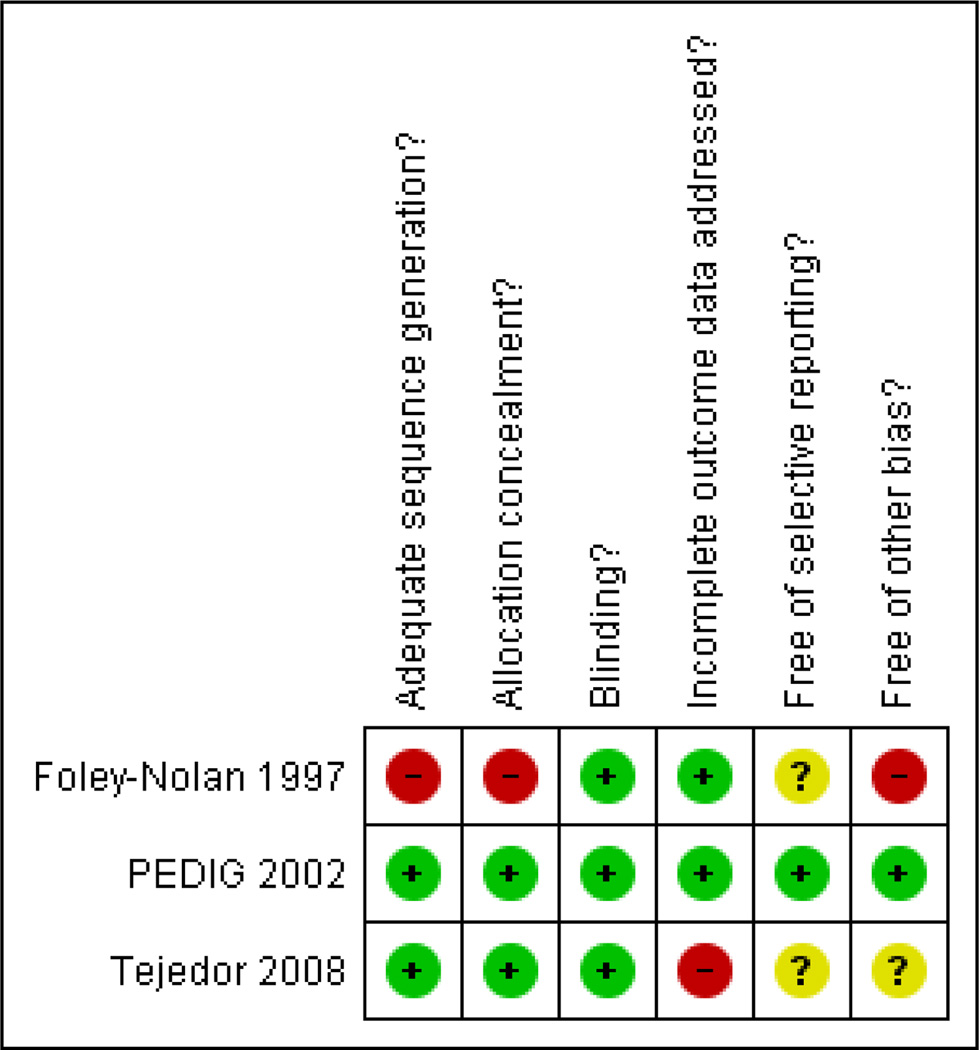
Main results: Three trials with a total of 525 amblyopic eyes were included. One trial was assessed as having a low risk of bias among these three trials, and one was assessed as having a high risk of bias.Evidence from three trials suggests atropine penalization is as effective as conventional occlusion. One trial found similar improvement in vision at six and 24 months. At six months, visual acuity in the amblyopic eye improved from baseline 3.16 lines in the occlusion and 2.84 lines in the atropine group (mean difference 0.034 logMAR; 95% confidence interval (CI) 0.005 to 0.064 logMAR). At 24 months, additional improvement was seen in both groups; but there continued to be no meaningful difference (mean difference 0.01 logMAR; 95% CI -0.02 to 0.04 logMAR). The second trial reported atropine to be more effective than occlusion. At six months, visual acuity improved 1.8 lines in the patching group and 3.4 lines in the atropine penalization group, and was in favor of atropine (mean difference -0.16 logMAR; 95% CI -0.23 to -0.09 logMAR). Different occlusion modalities were used in these two trials. The third trial had inherent methodological flaws and limited inference could be drawn.No difference in ocular alignment, stereo acuity and sound eye visual acuity between occlusion and atropine penalization was found. Although both treatments were well tolerated, compliance was better in atropine. Atropine penalization costs less than conventional occlusion. The results indicate that atropine penalization is as effective as conventional occlusion.
Authors' conclusions: Both conventional occlusion and atropine penalization produce visual acuity improvement in the amblyopic eye. Atropine penalization appears to be as effective as conventional occlusion, although the magnitude of improvement differed among the three trials. Atropine penalization can be used as first line treatment for amblyopia.
Figures
References
References to studies
Included studies
-
-
Foley-Nolan 1997 Foley-Nolan A, McCann A, O'Keefe M. Atropine penalisation versus occlusion as the primary treatment for amblyopia. British Journal of Ophthalmology. 1997;81(1):54–57.
-
-
-
PEDIG 2002 Hertle RW, Scheiman MM, Beck RW, Chandler DL, Bacal DA, Birch E, et al. Pediatric Eye Disease Investigator Group. Stability of visual acuity improvement following discontinuation of amblyopia treatment in children aged 7 to 12 years. Archives of Ophthalmology. 2007;125(5):655–659. Holmes JM, Beck RW, Kraker RT, Astle WF, Birch EE, Cole SR, et al. Pediatric Eye Disease Investigator Group. Risk of amblyopia recurrence after cessation of treatment. Journal of AAPOS. 2004;8(5):420–428. Holmes JM, Beck RW, Kraker RT, Cole SR, Repka MX, Birch EE, et al. Pediatric Eye Disease Investigator Group. Impact of patching and atropine treatment on the child and family in the amblyopia treatment study. Archives of Ophthalmology. 2003;121(11):1625–1632. Pediatric Eye Disease Investigator Group. Repka MX, Kraker RT, Beck RW, Holmes JM, Cotter SA, Birch EE, et al. A randomized trial of atropine vs patching for treatment of moderate amblyopia: follow-up at age 10 years. Archives of Ophthalmology. 2008;126(8):1039–1044. Pediatric Eye Disease Investigator Group. A comparison of atropine and patching treatments for moderate amblyopia by patient age, cause of amblyopia, depth of amblyopia, and other factors. Ophthalmology. 2003;110(8):1632–1637. Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Archives of Ophthalmology. 2002;120(3):268–278. Pediatric Eye Disease Investigator Group. The clinical profile of moderate amblyopia in children younger than 7 years. Archives of Ophthalmology. 2002;120(3):281–287. Pediatric Eye Disease Investigator Group. The course of moderate amblyopia treated with atropine in children: experience of the amblyopia treatment study. American Journal of Ophthalmology. 2003;136(4):630–639. Pediatric Eye Disease Investigator Group. The course of moderate amblyopia treated with patching in children: experience of the amblyopia treatment study. American Journal of Ophthalmology. 2003;136(4):620–629. Repka MX, Melia M, Eibschitz-Tsimhoni M, London R, Magoon E. Pediatric Eye Disease Investigator Group. The effect on refractive error of unilateral atropine as compared with patching for the treatment of amblyopia. Journal of AAPOS. 2007;11(3):300–302. Repka MX, Holmes JM, Melia BM, Beck RW, Gearinger MD, Tamkins SM, et al. Pediatric Eye Disease Investigator Group. The effect of amblyopia therapy on ocular alignment. Journal of AAPOS. 2005;9(6):542–545. Repka MX, Wallace DK, Beck RW, Kraker RT, Birch EE, Cotter SA, et al. Pediatric Eye Disease Investigator Group. Twoyear follow-up of a 6-month randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Archives of Ophthalmology. 2005;123(2):149–157.
-
-
-
Tejedor 2008 Published and unpublished data [ISRCTN: ISRCTN89210627] Tejedor J, Ogallar C. Comparative efficacy of penalization methods in moderate to mild amblyopia. American Journal of Ophthalmology. 2008;145(3):562–569.
-
Excluded studies
-
-
Chatzistefanou 2000 Chatzistefanou KI, Mills MD. The role of drug treatment in children with strabismus and amblyopia. Paediatric Drugs. 2000;2(2):91–100.
-
-
-
Cole 2001 Cole SR, Beck RW, Moke PS, Celano MP, Drews CD, Repka MX, et al. Pediatric Eye Disease Investigator Group. The Amblyopia Treatment Index. Journal of AAPOS. 2001;5(4):250–254.
-
-
-
Sheiman 2005 Scheiman MM, Hertle RW, Beck RW, Edwards AR, Birch E, Cotter SA, et al. Pediatric Eye Disease Investigator Group. Randomized trial of treatment of amblyopia in children aged 7 to 17 years. Archives of Ophthalmology. 2005;123(4):437–447.
-
-
-
Wu 2006 Wu C, Hunter DG. Amblyopia: diagnostic and therapeutic options. American Journal of Ophthalmology. 2006;141(1):175–184.
-
Studies awaiting classification
-
-
Menon 2008 Menon V, Shailesh G, Sharma P, Saxena R. Clinical trial of patching versus atropine penalization for the treatment of anisometropic amblyopia in older children. Journal of AAPOS. 2008;12(5):493–497.
-
-
-
PEDIG 2008 [ClinicalTrials.gov: NCT00315328] Scheiman MM, Hertle RW, Kraker RT, Beck RW, Birch EE, Felius J, et al. Pediatric Eye Disease Investigator Group. Patching vs atropine to treat amblyopia in children aged 7 to 12 years: a randomized trial. Archives of Ophthalmology. 2008;126(12):1634–1642.
-
-
-
Yan 2008 Yan JJ, Peng HC, Wu CX, Liu ZY, Wang YF. A clinical trial of atropine penalization vs patching for treatment of monocular amblyopia. International Journal of Ophthalmology. 2008;8(4):777–778.
-
Other references
Additional references
-
-
AAO 2007 American Academy of Ophthalmology Pediatric Ophthalmology/Strabismus Panel. Preferred Practice Pattern®=Guidelines. Amblyopia. http://www.aao.org/ppp.
-
-
-
Ansons 2001 Ansons A, Davis H. Diagnosis and Management of Ocular Motility Disorders. 3rd edition. Oxford: Blackwell Science; 2001.
-
-
-
Antonio-Santos 2006 Antonio-Santos A, Vedula SS, Hatt SR, Powell C. Interventions for stimulus deprivation amblyopia. Cochrane Database of Systematic Reviews. 2006;(Issue 3) Art. No.: CD005136.
-
-
-
AOA 1997 Rouse MW, Cooper JS, Cotter SA, Press LJ, Tannen BM. Care Of the patient with amblyopia: reference guide for clinicians. 1997 http://www.aoa.org/documents/CPG-4.pdf.
-
-
-
Attebo 1998 Attebo K, Mitchell P, Cumming R, Smith W, Jolly N, Sparkes R. Prevalence and causes of amblyopia in an adult population. Ophthalmology. 1998;105(1):154–159.
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical