

Routine pre-pregnancy health promotion for improving pregnancy outcomes
- PMID: 19821424
- PMCID: PMC4164828
- DOI: 10.1002/14651858.CD007536.pub2
Routine pre-pregnancy health promotion for improving pregnancy outcomes
Abstract
Background: A number of potentially modifiable risk factors are known to be associated with poor pregnancy outcomes. These include smoking, drinking excess alcohol, and poor nutrition. Routine health promotion (encompassing education, advice and general health assessment) in the pre-pregnancy period has been proposed for improving pregnancy outcomes by encouraging behavioural change, or allowing early identification of risk factors. While results from observational studies have been encouraging, this review examines evidence from randomised controlled trials of preconception health promotion.
Objectives: To assess the effectiveness of routine pre-pregnancy health promotion for improving pregnancy outcomes when compared with no pre-pregnancy care or usual care.
Search strategy: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (February 2009).
Selection criteria: Randomised and quasi-randomised trials examining health promotion interventions which aim to identify and modify risk factors before pregnancy. The review focuses on all women of childbearing age rather than those in high-risk groups. We have excluded trials where interventions are aimed specifically at women with established medical, obstetric or genetic risks or already receiving treatment as part of programmes for high-risk groups.
Data collection and analysis: Two review authors independently assessed eligibility and carried out data extraction.
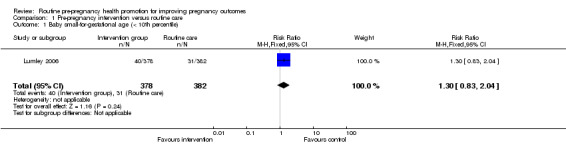
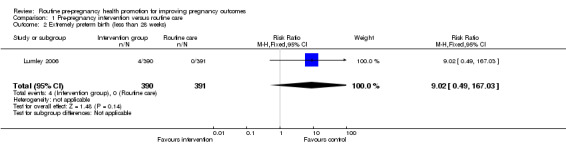
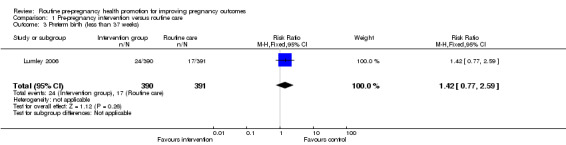
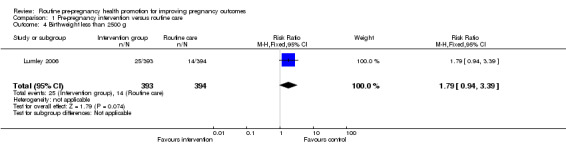
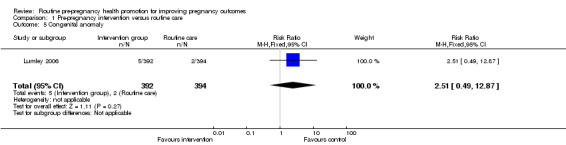
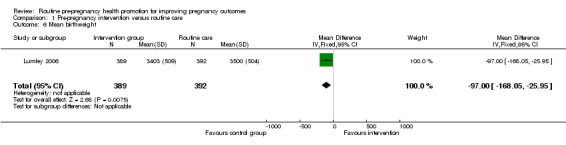
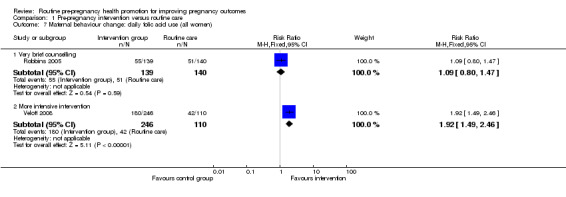
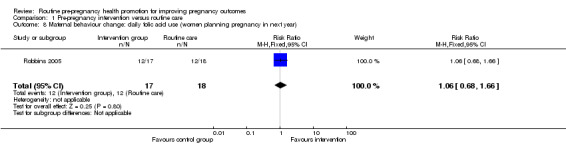
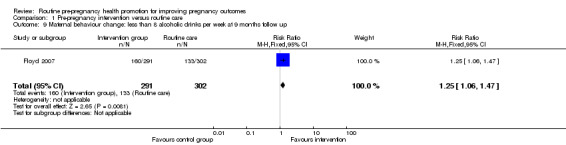
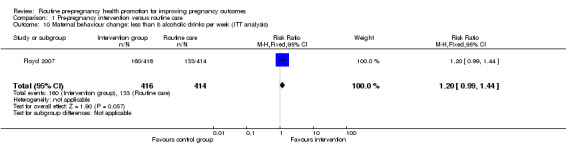
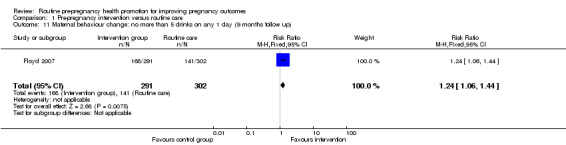
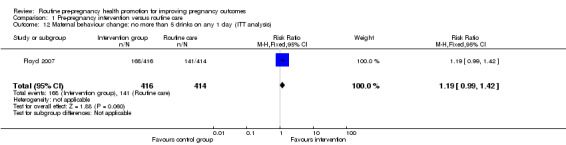
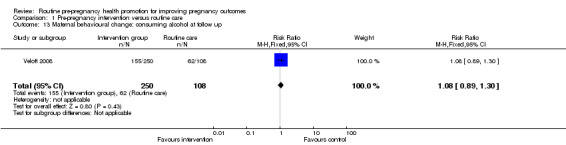
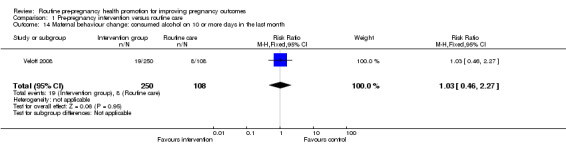
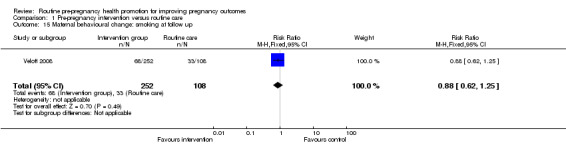
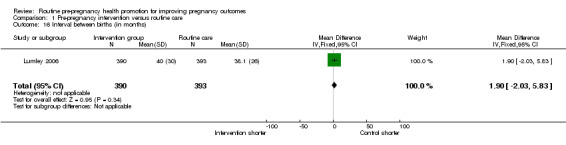
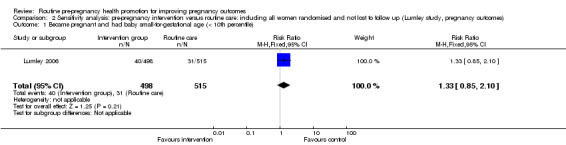
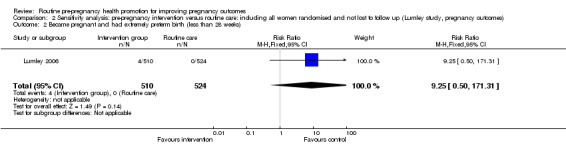
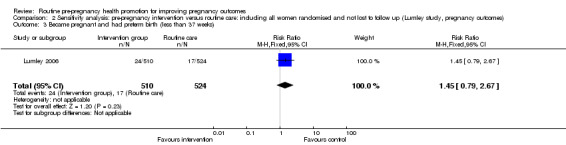
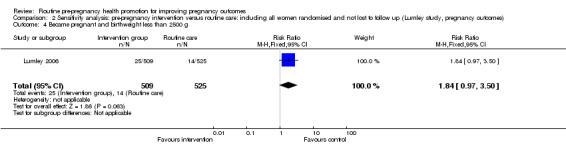
Main results: Four trials (2300 women) are included. The interventions ranged from brief advice through to education on health and lifestyle over several sessions. For most outcomes, data were only available from individual studies. Only one study followed up through pregnancy and there was no strong evidence of a difference between groups for preterm birth, congenital anomalies or weight for gestational age; only one finding (mean birthweight) reached statistical significance (mean difference -97.00, 95% confidence interval (CI) -168.05 to -25.95). This finding needs to be interpreted with caution as pregnancy outcome data were available for only half of the women randomised. There was some evidence that health promotion interventions were associated with positive maternal behavioural change including lower rates of binge drinking (risk ratio 1.24, 95% CI 1.06 to 1.44). Overall, there has been little research in this area and there is a lack of evidence on the effects of pre-pregnancy health promotion on pregnancy outcomes.
Authors' conclusions: There is little evidence on the effects of pre-pregnancy health promotion and much more research is needed in this area. There is currently insufficient evidence to recommend the widespread implementation of routine pre-pregnancy health promotion for women of childbearing age, either in the general population or between pregnancies.
Conflict of interest statement
None known.
Figures
Comment in
-
Little evidence from randomised controlled trials regarding effects of routine health promotion interventions for pregnant women.Evid Based Nurs. 2010 Feb;13(1):20-1. doi: 10.1136/ebn1028. Evid Based Nurs. 2010. PMID: 20179064 No abstract available.
References
References to studies included in this review
Elsinga 2006 {published and unpublished data}
Floyd 2007 {published data only}
-
- Ceperich S, Ingersoll K, Kareakashian M, Penberthy JK, Farrell L, Fabbri S, et al. Early outcomes of a 1‐session intervention to prevent alcohol‐exposed pregnancy in preconception women. Proceedings of the 70th Annual Scientific Meeting of the College on Problems of Drug Dependence; 2008 June 14‐19; San Juan, Puerto Rico. 2008:32.
Jack 1998 {published and unpublished data}
-
- Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing preconception risks identified at the time of a negative pregnancy test. A randomized trial. Journal of Family Practice 1998;47(1):33‐8. - PubMed
Lumley 2006 {published and unpublished data}
-
- Lumley J. A randomized trial of pre‐pregnancy counselling in inner city Melbourne. Personal communication 1993.
Robbins 2005 {published and unpublished data}
-
- Robbins JM, Cleves MA, Collins HB, Andrews N, Smith LN, Hobbs CA. Randomized trial of a physician‐based intervention to increase the use of folic acid supplements among women. American Journal of Obstetrics & Gynecology 2005;192(4):1126‐32. - PubMed
Velott 2008 {published and unpublished data}
-
- Velott DL, Baker SA, Hillemeier MM, Weisman CS. Participant recruitment to a randomized trial of a community‐based behavioral intervention for pre‐ and interconceptional women findings from the Central Pennsylvania Women's Health Study. Womens Health Issues 2008;18(3):217‐24. - PubMed
References to studies excluded from this review
Prunty 2008 {published data only}
-
- Prunty MC, Sharpe L, Butow P, Fulcher G. The motherhood choice: a decision aid for women with multiple sclerosis. Patient Education and Counseling 2008;71(1):108‐15. - PubMed
Additional references
Adams 1993
-
- Adams MM, Bruce FC, Shulman HB, Kendrick JS, Brogan DJ. Pregnancy planning and pre‐conception counseling. The PRAMS Working Group. Obstetrics & Gynecology 1993;82(6):955‐9. - PubMed
Clark 1994
-
- Clark NA, Fisk NM. Minimal compliance with the Department of Health recommendation for routine folate prophylaxis to prevent fetal neural tube defects. British Journal of Obstetrics and Gynaecology 1994;101(8):709‐10. - PubMed
Czeizel 1999
-
- Czeizel AE. Ten years of experience in periconceptional care. European Journal of Obstetrics & Gynecology and Reproductive Biology 1999;84(1):43‐9. - PubMed
de Jong‐Potjer 2003
-
- Jong‐Potjer LC, Bock GH, Zaadstra BM, Jong ORW, Verloove‐Vanhorick SP, Springer MP. Women's interest in GP‐initiated pre‐conception counselling in The Netherlands. Family Practice 2003;20(2):142‐6. - PubMed
Deeks 2001
-
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic reviews in health care: meta‐analysis in context. London: BMJ Books, 2001.
Evers 2002
-
- Evers JL. Female subfertility. Lancet 2002;360:151‐9. - PubMed
Gates 2005
-
- Gates S. Methodological Guidelines. In: The Editorial Team. Pregnancy and Childbirth Group. About the Cochrane Collaboration (Collaborative Review Groups (CRGs)) 2005, Issue 2 .
Gnoth 2003
-
- Gnoth C, Frank‐Herrmann P, Freundl G, Godehardt D, Godehardt E. Time to pregnancy: results of the German prospective study and impact on the management of infertility. Human Reproduction 2003;18:1959‐66. - PubMed
Heyes 2004
-
- Heyes T, Long S, Mathers N. Preconception care: practice and beliefs of primary care workers. Family Practice 2004;21(1):22‐7. - PubMed
Higgins 2008
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Johnson 2006
-
- Johnson K, Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to improve preconception health and health care‐‐United States. A report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. Morbidity and Mortality Weekly Reports 2006;55(RR‐6):1‐23. - PubMed
RCOG 2008
-
- RCOG, RCM, RCA, RCPCH. Standards for maternity care. Report of a Working Party. London: RCOG Press, 2008.
RevMan 2008 [Computer program]
-
- The Cochrane Collaboration. Review Manager (RevMan). Version 5.0. Copenhagen, The Nordic Cochrane Centre: The Cochrane Collaboration, 2008.
Stade 2009
-
- Stade BC, Bailey C, Dzendoletas D, Sgro M. Dowswell T. Psychological and/or educational interventions for reducing prenatal alcohol consumption in pregnant women and women planning pregnancy. Cochrane Database of Systematic Reviews 2009, Issue 2. [DOI: 10.1002/14651858.CD004228] - DOI - PMC - PubMed
Tieu 2009
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical