

Urate as a predictor of the rate of clinical decline in Parkinson disease
- PMID: 19822770
- PMCID: PMC2795011
- DOI: 10.1001/archneurol.2009.247
Urate as a predictor of the rate of clinical decline in Parkinson disease
Abstract
Background: The risk of Parkinson disease (PD) and its rate of progression may decline with increasing concentration of blood urate, a major antioxidant.
Objective: To determine whether serum and cerebrospinal fluid concentrations of urate predict clinical progression in patients with PD.
Design, setting, and participants: Eight hundred subjects with early PD enrolled in the Deprenyl and Tocopherol Antioxidative Therapy of Parkinsonism (DATATOP) trial. The pretreatment urate concentration was measured in serum for 774 subjects and in cerebrospinal fluid for 713 subjects.
Main outcome measures: Treatment-, age-, and sex-adjusted hazard ratios (HRs) for clinical disability requiring levodopa therapy, the prespecified primary end point of the original DATATOP trial.
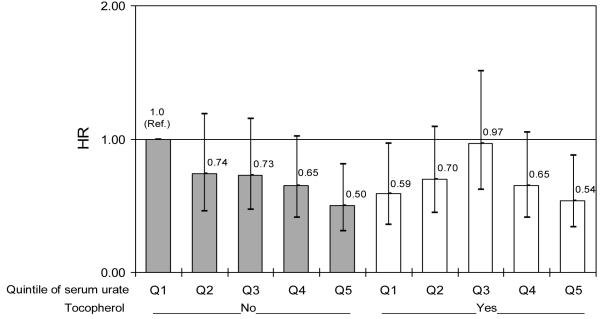
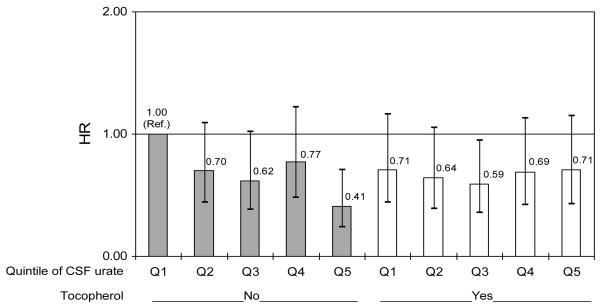
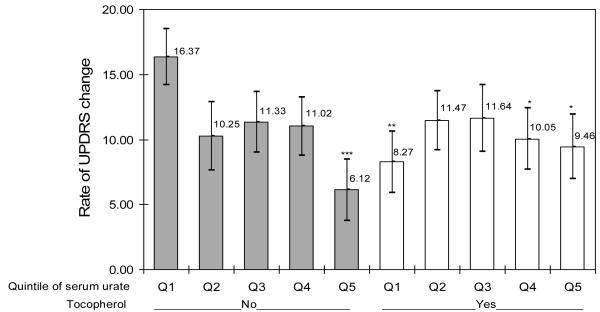
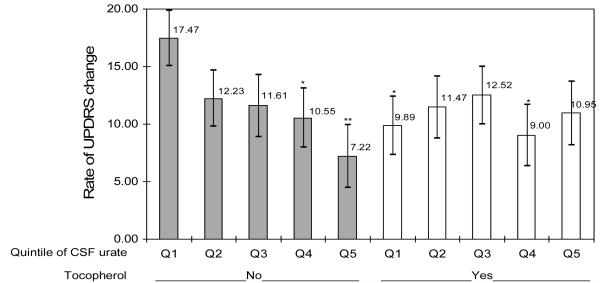
Results: The HR of progressing to the primary end point decreased with increasing serum urate concentrations (HR for highest vs lowest quintile = 0.64; 95% confidence interval [CI], 0.44-0.94; HR for a 1-SD increase = 0.82; 95% CI, 0.73-0.93). In analyses stratified by alpha-tocopherol treatment (2000 IU/d), a decrease in the HR for the primary end point was seen only among subjects not treated with alpha-tocopherol (HR for a 1-SD increase = 0.75; 95% CI, 0.62-0.89; vs HR for those treated = 0.90; 95% CI, 0.75-1.08). Results were similar for the rate of change in the Unified Parkinson's Disease Rating Scale score. Cerebrospinal fluid urate concentration was also inversely related to both the primary end point (HR for highest vs lowest quintile = 0.65; 95% CI, 0.44-0.96; HR for a 1-SD increase = 0.89; 95% CI, 0.79-1.02) and the rate of change in the Unified Parkinson's Disease Rating Scale score. As with serum urate concentration, these associations were present only among subjects not treated with alpha-tocopherol.
Conclusions: Higher serum and cerebrospinal fluid urate concentrations at baseline were associated with slower rates of clinical decline. The findings strengthen the link between urate concentration and PD and the rationale for considering central nervous system urate concentration elevation as a potential strategy to slow PD progression.
Figures
Comment in
-
Natural oxidant balance in Parkinson disease.Arch Neurol. 2009 Dec;66(12):1445. doi: 10.1001/archneurol.2009.261. Arch Neurol. 2009. PMID: 20008647 No abstract available.
References
-
- Alho H, Leinonen JS, Erhola M, Lonnrot K, Aejmelaeus R. Assay of antioxidant capacity of human plasma and CSF in aging and disease. Restor Neurol Neurosci. 1998;12:159–165. - PubMed
-
- Johnson RJ, Titte S, Cade JR, Rideout BA, Oliver WJ. Uric acid, evolution and primitive cultures. Semin Nephrol. 2005;25:3–8. - PubMed
-
- Burkhardt CR, Weber HK. Parkinson’s disease: a chronic, low-grade antioxidant deficiency? Med Hypotheses. 1994;43:111–114. - PubMed
-
- Beal MF. Mitochondria take center stage in aging and neurodegeneration. Ann Neurol. 2005;58:495–505. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
