

Patterns of relapse and prognosis after bevacizumab failure in recurrent glioblastoma
- PMID: 19822869
- PMCID: PMC2839807
- DOI: 10.1212/WNL.0b013e3181bc0184
Patterns of relapse and prognosis after bevacizumab failure in recurrent glioblastoma
Abstract
Background: Bevacizumab has recently been approved by the US Food and Drug Administration for recurrent glioblastoma (GBM). However, patterns of relapse, prognosis, and outcome of further therapy after bevacizumab failure have not been studied systematically.
Methods: We identified patients at Memorial Sloan-Kettering Cancer Center with recurrent GBM who discontinued bevacizumab because of progressive disease.
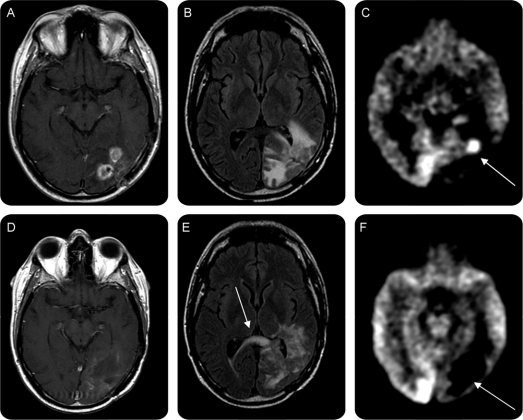
Results: There were 37 patients (26 men with a median age of 54 years). The most common therapies administered concurrently with bevacizumab were irinotecan (43%) and hypofractionated reirradiation (38%). The median overall survival (OS) after progressive disease on bevacizumab was 4.5 months; 34 patients died. At the time bevacizumab was discontinued for tumor progression, 17 patients (46%) had an increase in the size of enhancement at the initial site of disease (local recurrence), 6 (16%) had a new enhancing lesion outside of the initial site of disease (multifocal), and 13 (35%) had progression of predominantly nonenhancing tumor. Factors associated with shorter OS after discontinuing bevacizumab were lower performance status and nonenhancing pattern of recurrence. Additional salvage chemotherapy after bevacizumab failure was given to 19 patients. The median progression-free survival (PFS) among these 19 patients was 2 months, the median OS was 5.2 months, and the 6-month PFS rate was 0%.
Conclusions: Contrast enhanced MRI does not adequately assess disease status during bevacizumab therapy for recurrent glioblastoma (GBM). A nonenhancing tumor pattern of progression is common after treatment with bevacizumab for GBM and is correlated with worse survival. Treatments after bevacizumab failure provide only transient tumor control.
Figures
Comment in
-
Patterns of relapse and prognosis after bevacizumab failure in recurrent glioblastoma.Neurology. 2010 Apr 13;74(15):1239-41. doi: 10.1212/WNL.0b013e3181d8a293. Neurology. 2010. PMID: 20385899 No abstract available.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–996. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol 1999;17:2572–2578. - PubMed
-
- Lamszus K, Ulbricht U, Matschke J, Brockmann MA, Fillbrandt R, Westphal M. Levels of soluble vascular endothelial growth factor (VEGF) receptor 1 in astrocytic tumors and its relation to malignancy, vascularity, and VEGF-A. Clin Cancer Res 2003;9:1399–1405. - PubMed
-
- Plate KH, Breier G, Weich HA, Risau W. Vascular endothelial growth factor is a potential tumour angiogenesis factor in human gliomas in vivo. Nature 1992;359:845–848. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical