

Correlation of enzyme-inducing anticonvulsant use with outcome of patients with glioblastoma
- PMID: 19822870
- PMCID: PMC2764724
- DOI: 10.1212/WNL.0b013e3181bbfeca
Correlation of enzyme-inducing anticonvulsant use with outcome of patients with glioblastoma
Abstract
Background: Clinical trials involving patients with glioblastoma (GBM) distinguish cohorts who are treated with enzyme-inducing anticonvulsants (EIAC). Such anticonvulsants induce hepatic P450 microsomal enzymes, which accelerate the metabolism of certain chemotherapy and molecular targeted agents. However, the resultant effect of such induction on patient outcome has received limited study.
Methods: We performed a correlative analysis of baseline EIAC use with outcome, using a cross-sectional database of 620 patients with newly diagnosed GBM treated prospectively on North Central Cancer Treatment Group trials.
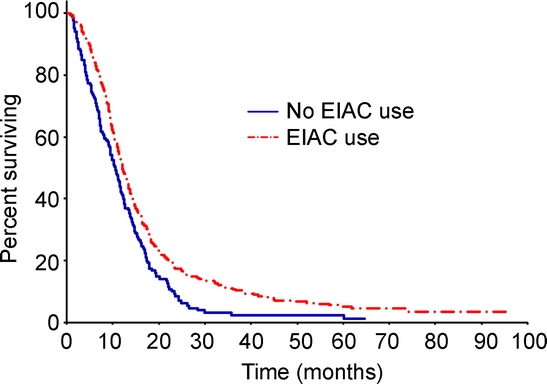
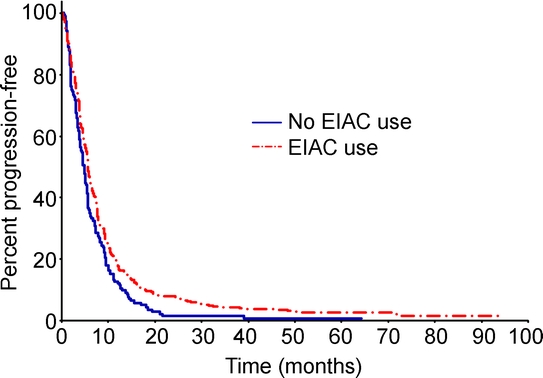
Results: At registration, 72% were receiving treatment with EIAC; 2% were receiving non-EIACs, and the 26% were not receiving anticonvulsants (26%). Surprisingly, in the multivariable Cox model, overall survival (OS) and progression-free survival (PFS) showed a positive correlation with EIAC use (hazard ratio [HR] = 0.75, p = 0.0028 and HR = 0.80, p = 0.022), even after adjustment for the known prognostic factors of age, performance status, extent of resection, steroid use, and baseline neurocognitive function. Specifically, the median OS was longer in EIAC compared with non-EIAC patients (12.3 vs 10.7 months, p = 0.0002). Similarly, PFS was longer in EIAC patients (5.6 vs 4.8 months, p = 0.003). No differences in median OS or PFS were observed when comparing patients with or without a history of seizures at baseline.
Conclusions: Paradoxically, enzyme-inducing anticonvulsant (EIAC) use correlated with superior outcome of patients with glioblastoma. These results suggest that in comparative clinical trials testing agents metabolized by P450 microsomal enzymes, treatment arms may need stratification for the proportion of patients receiving EIAC.
Figures
Comment in
-
Correlation of enzyme-inducing anticonvulsant use with outcome of patients with glioblastoma.Neurology. 2010 Apr 20;74(16):1329; author reply 1329-30. doi: 10.1212/WNL.0b013e3181d8a5ed. Neurology. 2010. PMID: 20404315 No abstract available.
-
Correlation of enzyme-inducing anticonvulsant use with outcome of patients with glioblastoma.Neurology. 2010 Apr 20;74(16):1330-1; author reply 1331. doi: 10.1212/WNL.0b013e3181d8a5c2. Neurology. 2010. PMID: 20404316 No abstract available.
References
-
- Relling MV, Pui CH, Sandlund JT, et al. Adverse effect of anticonvulsants on efficacy of chemotherapy for acute lymphoblastic leukaemia. Lancet 2000;356:285–290. - PubMed
-
- Buckner JC, Ballman KV, Michalak JC, et al. Phase III trial of carmustine and cisplatin compared with carmustine alone and standard radiation therapy or accelerated radiation therapy in patients with glioblastoma multiforme: North Central Cancer Treatment Group 93–72-52 and Southwest Oncology Group 9503 Trials. J Clin Oncol 2006;24:3871–3879. - PubMed
-
- Moynihan TJ, O’Fallon JR, Krook JE, et al. A phase II trial of pre-irradiation chemotherapy with BCNU, cisplatin and oral etoposide combined with radiation therapy in the treatment of glioblastoma (GBM). Program/Proceedings of the American Society of Clinical Oncology 2002;21:77a. Abstract 306.
-
- Uhm JH, Ballman KV, Krause JC, et al. Phase II study of ZD1839 in patients with newly diagnosed grade 4 astrocytoma. Program/Proceedings of the American Society of Clinical Oncology 2004;22:108s. Abstract 1505.
-
- Agresti A. Categorical Data Analysis. New York: John Wiley & Sons; 1990.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical