

Intraoperative use of handheld spectral domain optical coherence tomography imaging in macular surgery
- PMID: 19823107
- PMCID: PMC3515871
- DOI: 10.1097/IAE.0b013e3181b266bc
Intraoperative use of handheld spectral domain optical coherence tomography imaging in macular surgery
Erratum in
- Retina. 2011 Jun;31(6):1236
Abstract
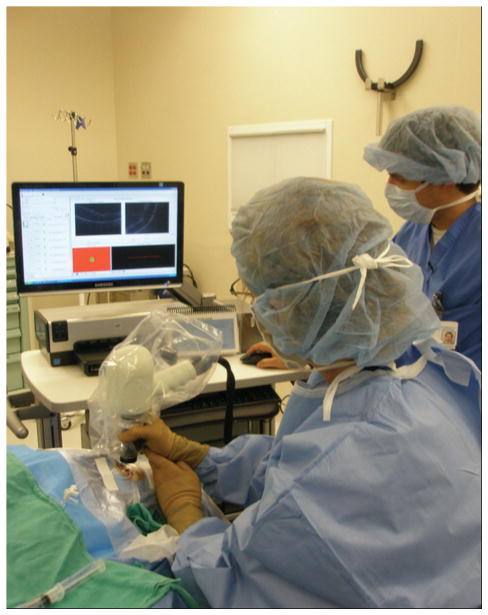
Purpose: To describe the intraoperative use of handheld spectral domain optical coherence tomography (SDOCT) imaging in macular surgery.
Design: Prospective, observational case series.
Methods: A handheld SDOCT device was used to obtain preincision optical coherence tomography imaging in patients undergoing vitrectomy for macular diseases. After removal of the internal limiting membrane or the epiretinal membrane, repeat intraoperative imaging was obtained. Spectral domain optical coherence tomography findings were characterized.
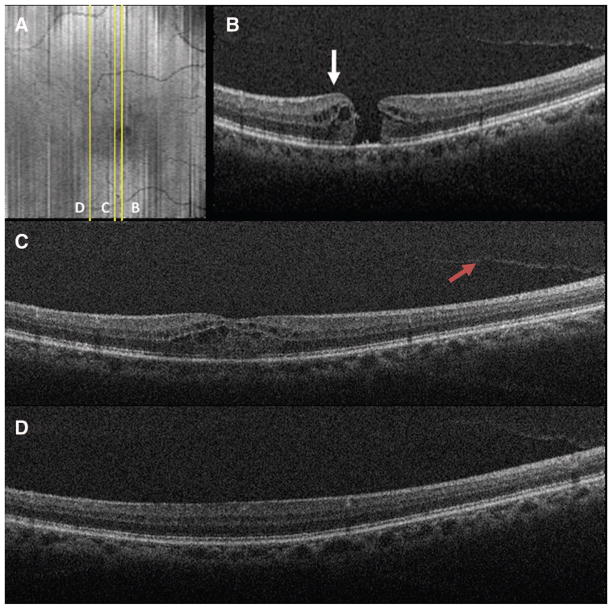
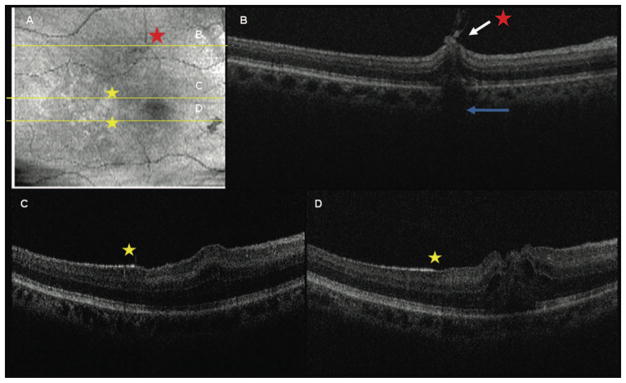
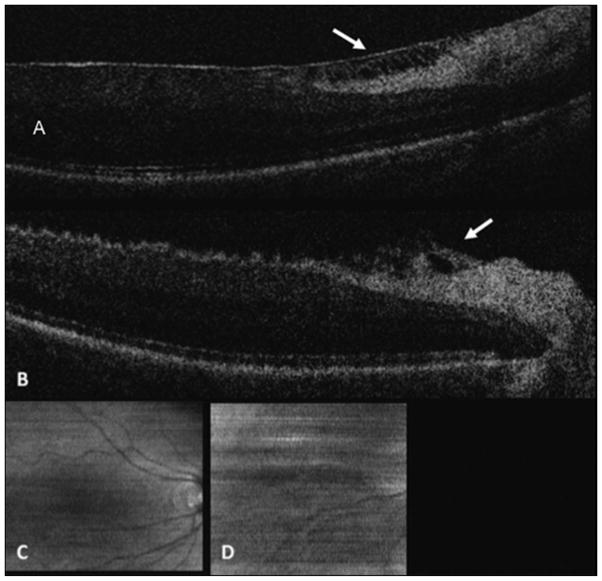
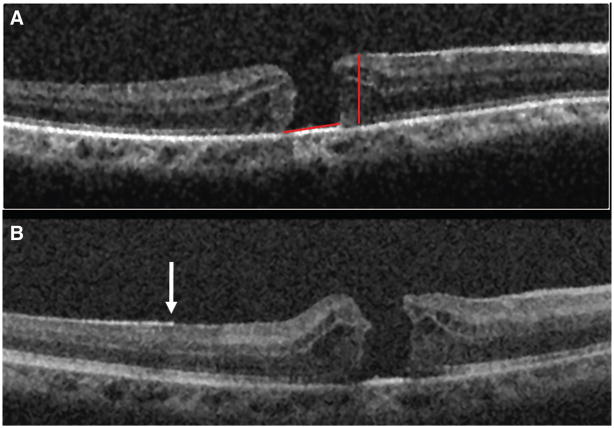
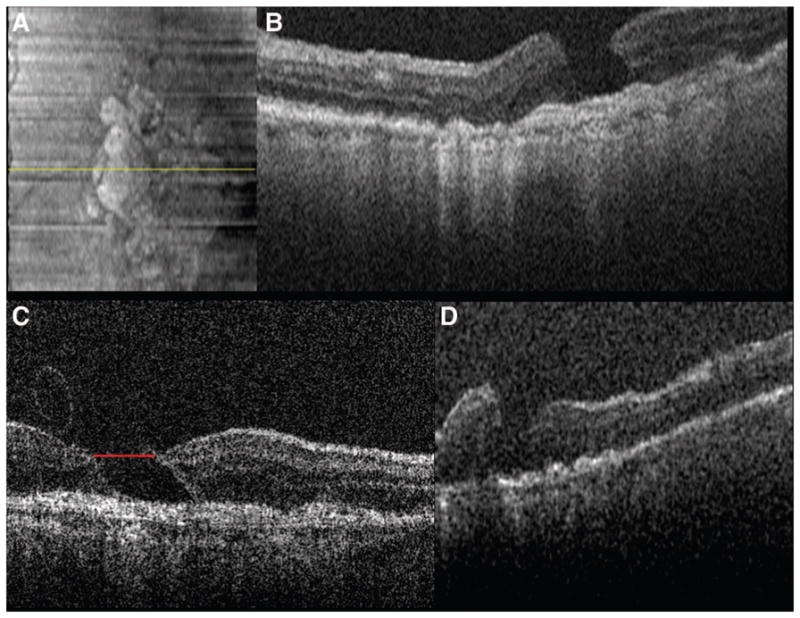
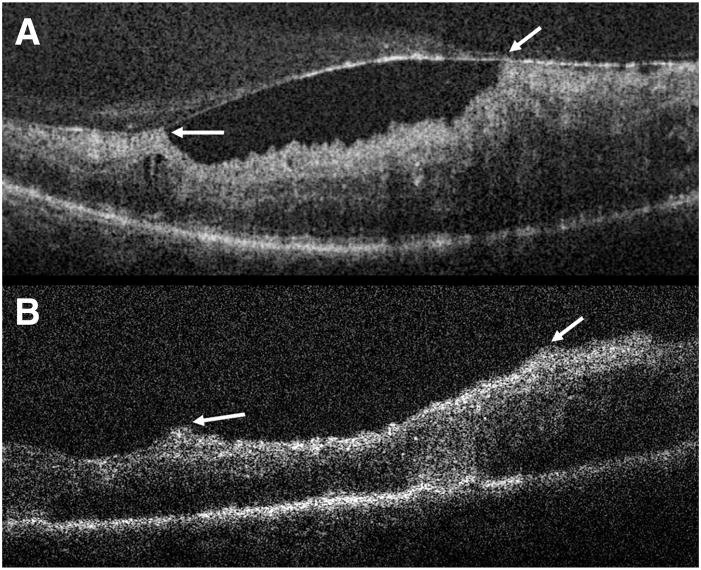
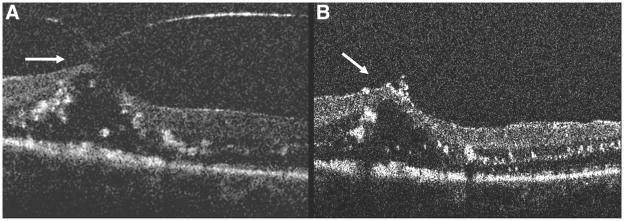
Results: An efficient technique was established for obtaining intraoperative SDOCT imaging. A total of eight patients were included in the study. Four patients underwent surgery for macular hole, three patients for epiretinal membrane, and one for vitreomacular traction. Comparison of the preincision and intraoperative SDOCT images demonstrated distinct changes in retinal contour and macular hole configuration. Intraoperative SDOCT imaging identified additional membranes in two patients.
Conclusion: The intraoperative use of handheld SDOCT imaging provides an efficient method for visualizing macular pathology. This technology may, in certain cases, help confirm or identify diseases that may be difficult to visualize during surgery.
Figures
References
-
- Hee MR, Puliafito CA, Wong C, et al. Optical coherence tomography of macular holes. Ophthalmology. 1995;102:748–756. - PubMed
-
- Gaudric A, Haouchine B, Massin P, Paques M, Blain P, Erginay A. Macular hole formation: new data provided by optical coherence tomography. Arch Ophthalmol. 1999;117:744–751. - PubMed
-
- Puliafito CA, Hee MR, Lin CP, et al. Imaging of macular diseases with optical coherence tomography. Ophthalmology. 1995;102:217–229. - PubMed
-
- Toth CA, Narayan DG, Boppart SA, et al. A comparison of retinal morphology viewed by optical coherence tomography and by light microscopy. Arch Ophthalmol. 1997;115:1425–1428. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
