

Combining radiation, immunotherapy, and antiangiogenesis agents in the management of cancer: the Three Musketeers or just another quixotic combination?
- PMID: 19823740
- PMCID: PMC6309404
- DOI: 10.1039/b911313b
Combining radiation, immunotherapy, and antiangiogenesis agents in the management of cancer: the Three Musketeers or just another quixotic combination?
Abstract
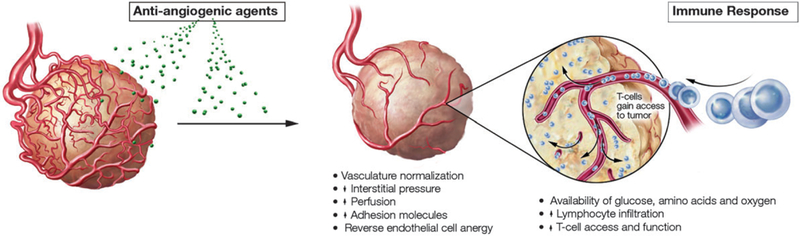
With the advent of new cancer therapies in the last few years, the goals of reducing disease burden and improving quality of life are frequently achieved. Yet despite the advances seen with numerous monotherapies, a multimodality approach that targets different aspects of tumor biology may yield the greatest clinical benefit for patients with late-stage disease. Many such strategies have been employed with varying degrees of success. The addition of immunotherapy to standard-of-care radiation therapy has shown evidence of efficacy in some preclinical models and in the clinical setting. However, exploiting these two modalities safely and effectively remains an ongoing challenge. It is feasible that the addition of another therapeutic modality could further enhance the antitumor effects of these treatments. The recent addition of angiogenesis inhibitors to the cancer treatment armamentarium represents an attractive option, especially since these agents have been shown to be most effective when combined with other therapies. This review examines preclinical and clinical data on the interaction between immunotherapy and radiation, and discusses the potential synergy between these two modalities and angiogenesis inhibitors.
Figures



References
-
- National Cancer Institute/NIH Available from: http://www.cancer.gov/.
-
- Radiation Therapy Oncology Group (RTOG). Phase III double-blind placebo-controlled trial of conventional concurrent chemoradiation and adjuvant temozolomide plus bevacizumab versus conventional concurrent chemoradiation and adjuvant temozolomide in patients with newly diagnosed glioblastoma Available from: http://www.rtog.org/members/protocols/0825/0825.pdf.
-
- Tol J, Koopman M, Cats A, Rodenburg CJ, Creemers GJ, Schrama JG, Erdkamp FL, Vos AH, van Groeningen CJ, Sinnige HA, Richel DJ, Voest EE, Dijkstra JR, Vink-Borger ME, Antonini NF, Mol L, van Krieken JH, Dalesio O and Punt CJ, N. Engl. J. Med, 2009, 360, 563–572. - PubMed
-
- Hecht JR, Mitchell E, Chidiac T, Scroggin C, Hagenstad C, Spigel D, Marshall J, Cohn A, McCollum D, Stella P, Deeter R, Shahin S and Amado RG, J. Clin. Oncol, 2009, 27, 672–680. - PubMed
-
- Gehrmann M, Marienhagen J, Eichholtz-Wirth H, Fritz E, Ellwart J, Jaattela M, Zilch T and Multhoff G, Cell Death Differ, 2005, 12, 38–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases