

Clinical benefits of a multivariate prediction model for bladder cancer: a decision analytic approach
- PMID: 19823979
- PMCID: PMC2785133
- DOI: 10.1002/cncr.24615
Clinical benefits of a multivariate prediction model for bladder cancer: a decision analytic approach
Erratum in
- Cancer. 2011 Aug 15;117(16):3867
Abstract
Background: It has been demonstrated that multivariate prediction models predict cancer outcomes more accurately than cancer stage; however, the effects of these models on clinical management are unclear. The objective of the current study was to determine whether a previously published multivariate prediction model for bladder cancer ("bladder nomogram") improved medical decision making when referral for adjuvant chemotherapy was used as a model.
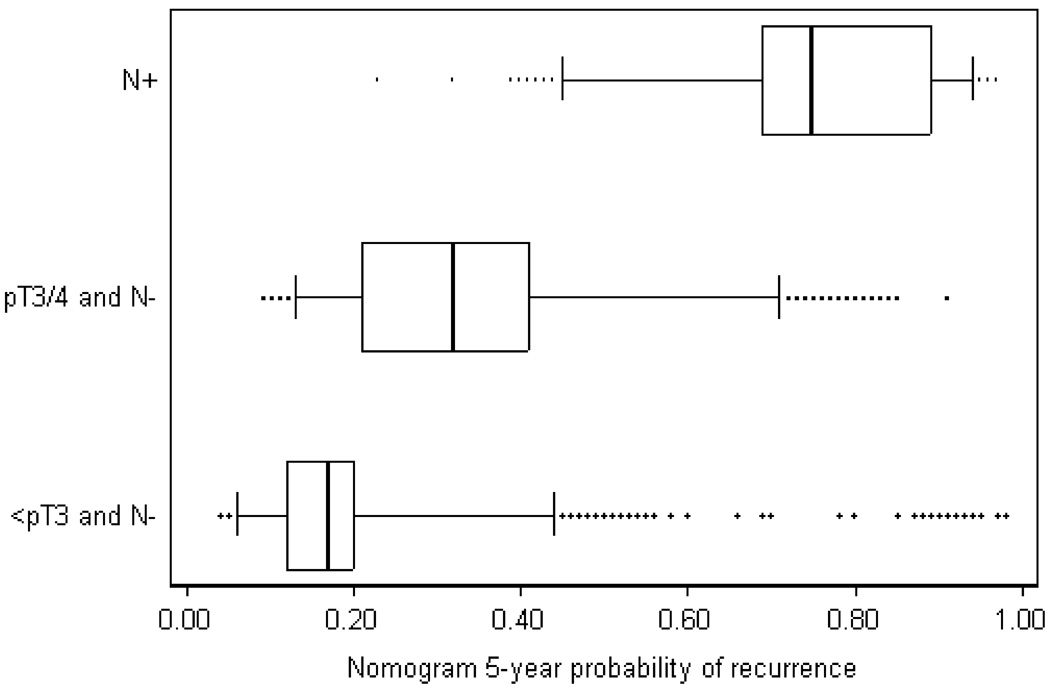
Methods: Data were analyzed from an international cohort study of 4462 patients who underwent cystectomy without chemotherapy from 1969 to 2004. The number of patients eligible for chemotherapy was determined using pathologic stage criteria (lymph node-positive disease or pathologic T3 [pT3] or pT4 tumor classification) and for 3 cutoff levels on the bladder nomogram (10%, 25%, and 70% risk of recurrence with surgery alone). The number of recurrences was calculated by applying a relative risk reduction to the baseline risk among eligible patients. Clinical net benefit was then calculated by combining recurrences and treatments and weighting the latter by a factor related to drug tolerability.
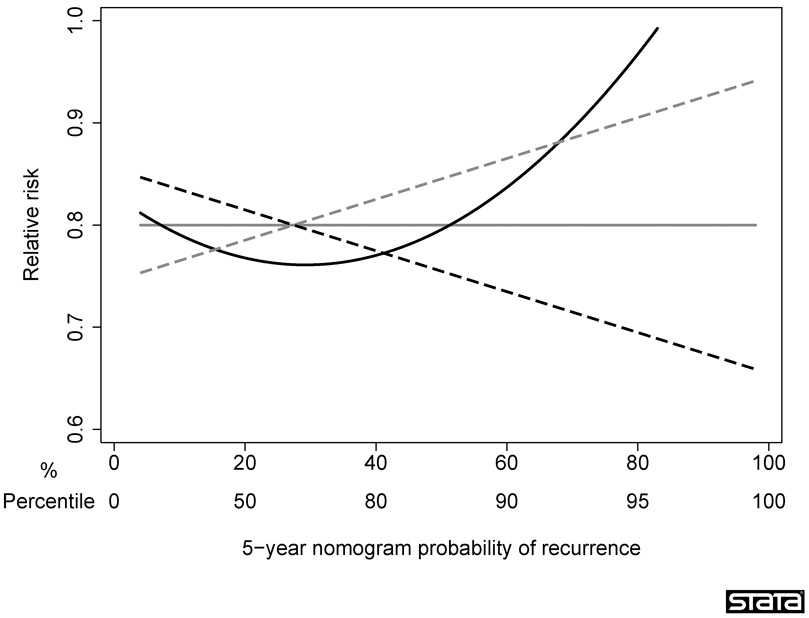
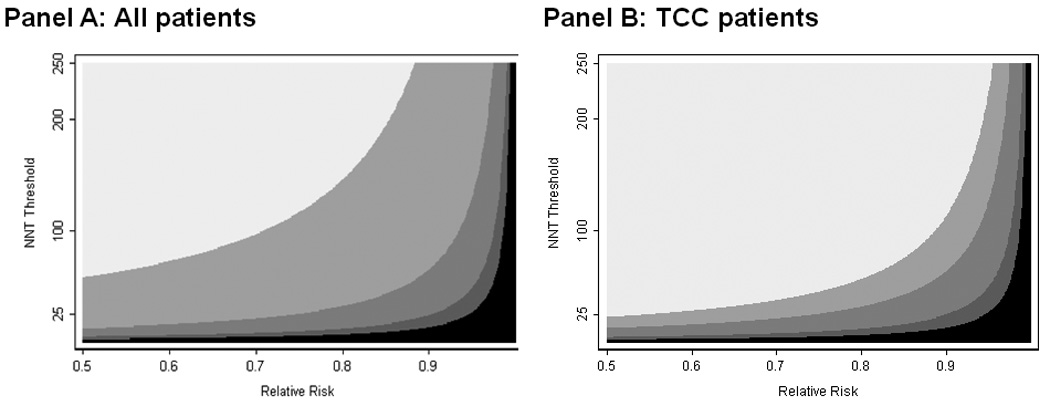
Results: A nomogram cutoff outperformed pathologic stage for chemotherapy in every scenario of drug effectiveness and tolerability. For a drug with a relative risk of 0.80, with which clinicians would treat <or=20 patients to prevent 1 recurrence, use of the nomogram was equivalent to a strategy that resulted in 60 fewer chemotherapy treatments per 1000 patients without any increase in recurrence rates.
Conclusions: The authors concluded that referring patients who undergo cystectomy to adjuvant chemotherapy on the basis of a multivariate model is likely to lead to better patient outcomes than the use of pathologic stage. Further research is warranted to evaluate the clinical effects of multivariate prediction models.
(c) 2009 American Cancer Society.
Conflict of interest statement
Conflict of interest statement
Andrew Vickers had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. None of the authors have any relevant conflicts of interest.
Figures
Comment in
-
Prognosis and prediction in a Facebook world.Cancer. 2009 Dec 1;115(23):5368-70. doi: 10.1002/cncr.24593. Cancer. 2009. PMID: 19658183 No abstract available.
-
Targeting chemotherapy to advanced bladder cancer patients most likely to benefit.Future Oncol. 2010 Feb;6(2):193-6. doi: 10.2217/fon.09.178. Future Oncol. 2010. PMID: 20146577
References
-
- Kanemitsu Y, Kato T, Hirai T, Yasui K. Preoperative probability model for predicting overall survival after resection of pulmonary metastases from colorectal cancer. Br J Surg. 2004;91(1):112–120. - PubMed
-
- Kattan MW, Karpeh MS, Mazumdar M, Brennan MF. Postoperative nomogram for disease-specific survival after an R0 resection for gastric carcinoma. J Clin Oncol. 2003;21(19):3647–3650. - PubMed
-
- Van Zee KJ, Manasseh DM, Bevilacqua JL, Boolbol SK, Fey JV, Tan LK, et al. A nomogram for predicting the likelihood of additional nodal metastases in breast cancer patients with a positive sentinel node biopsy. Ann Surg Oncol. 2003;10(10):1140–1151. - PubMed
-
- Karakiewicz PI, Briganti A, Chun FK, Trinh QD, Perrotte P, Ficarra V, et al. Multi-institutional validation of a new renal cancer-specific survival nomogram. J Clin Oncol. 2007;25(11):1316–1322. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
