

Incidence and mortality of hip fractures in the United States
- PMID: 19826027
- PMCID: PMC4410861
- DOI: 10.1001/jama.2009.1462
Incidence and mortality of hip fractures in the United States
Abstract
Context: Understanding the incidence and subsequent mortality following hip fracture is essential to measuring population health and the value of improvements in health care.
Objective: To examine trends in hip fracture incidence and resulting mortality over 20 years in the US Medicare population.
Design, setting, and patients: Observational study using data from a 20% sample of Medicare claims from 1985-2005. In patients 65 years or older, we identified 786,717 hip fractures for analysis. Medication data were obtained from 109,805 respondents to the Medicare Current Beneficiary Survey between 1992 and 2005.
Main outcome measures: Age- and sex-specific incidence of hip fracture and age- and risk-adjusted mortality rates.
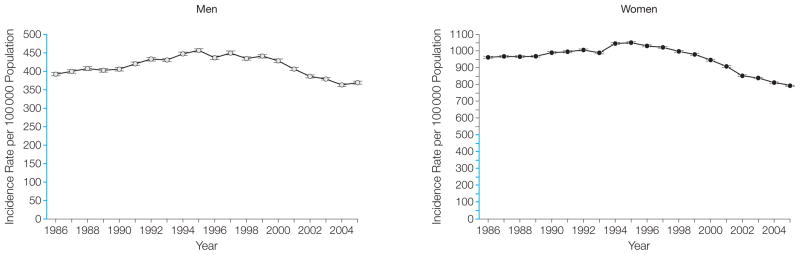
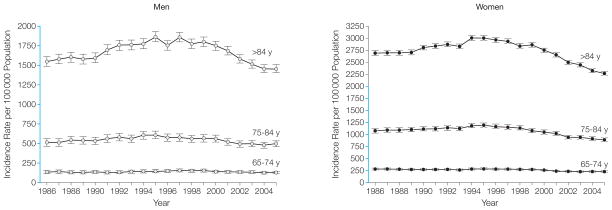
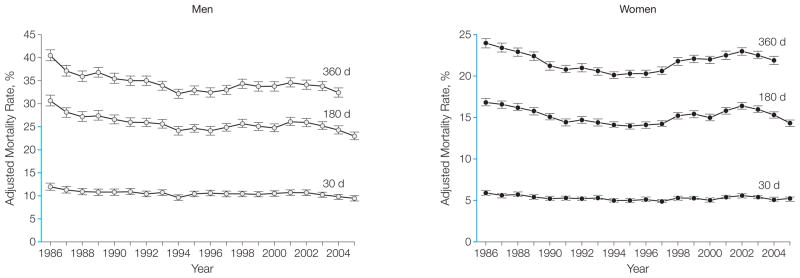
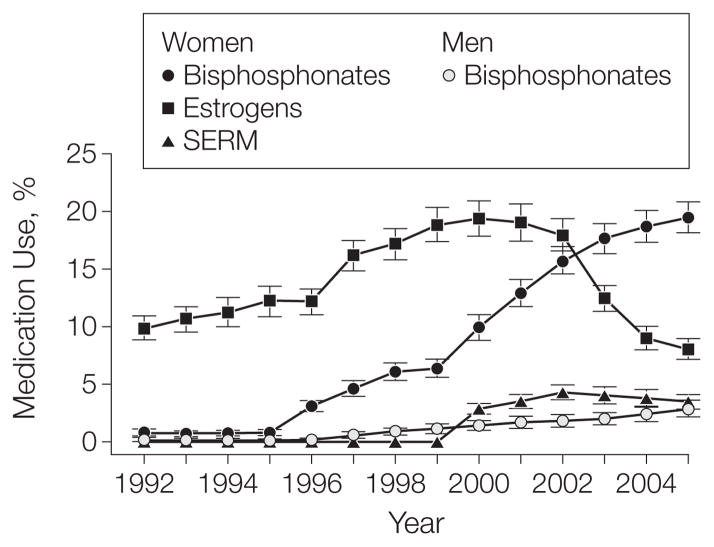
Results: Between 1986 and 2005, the annual mean number of hip fractures was 957.3 per 100,000 (95% confidence interval [CI], 921.7-992.9) for women and 414.4 per 100,000 (95% CI, 401.6-427.3) for men. The age-adjusted incidence of hip fracture increased from 1986 to 1995 and then steadily declined from 1995 to 2005. In women, incidence increased 9.0%, from 964.2 per 100,000 (95% CI, 958.3-970.1) in 1986 to 1050.9 (95% CI, 1045.2-1056.7) in 1995, with a subsequent decline of 24.5% to 793.5 (95% CI, 788.7-798.3) in 2005. In men, the increase in incidence from 1986 to 1995 was 16.4%, from 392.4 (95% CI, 387.8-397.0) to 456.6 (95% CI, 452.0-461.3), and the subsequent decrease to 2005 was 19.2%, to 369.0 (95% CI, 365.1-372.8). Age- and risk-adjusted mortality in women declined by 11.9%, 14.9%, and 8.8% for 30-, 180-, and 360-day mortality, respectively. For men, age- and risk-adjusted mortality decreased by 21.8%, 25.4%, and 20.0% for 30-, 180-, and 360-day mortality, respectively. Over time, patients with hip fracture have had an increase in all comorbidities recorded except paralysis. The incidence decrease is coincident with increased use of bisphosphonates.
Conclusion: In the United States, hip fracture rates and subsequent mortality among persons 65 years and older are declining, and comorbidities among patients with hip fractures have increased.
Figures
References
-
- Melton LJ, III, Gabriel SE, Crowson CS, Tosteson AN, Johnell O, Kanis JA. Cost-equivalence of different osteoporotic fractures. Osteoporos Int. 2003;14(5):383–388. - PubMed
-
- Hall SE, Williams JA, Senior JA, Goldswain PR, Criddle RA. Hip fracture outcomes: quality of life and functional status in older adults living in the community. Aust N Z J Med. 2000;30(3):327–332. - PubMed
-
- Randell AG, Nguyen TV, Bhalerao N, Silverman SL, Sambrook PN, Eisman JA. Deterioration in quality of life following hip fracture: a prospective study. Osteoporos Int. 2000;11(5):460–466. - PubMed
