

Odontoid process metastasis of bronchial carcinoma as a rare cause for nonmechanical neck pain: a case report
- PMID: 19830057
- PMCID: PMC2740268
- DOI: 10.4076/1757-1626-2-8173
Odontoid process metastasis of bronchial carcinoma as a rare cause for nonmechanical neck pain: a case report
Abstract
Introduction: About 10% of spinal metastases are found in the cervical level. Magnetic resonance imaging is the gold standard for early detection of spinal metastases. The decision whether cervical spine magnetic resonance imaging is requested or not must be made clinically, taking into consideration the patients' detailed pain history.
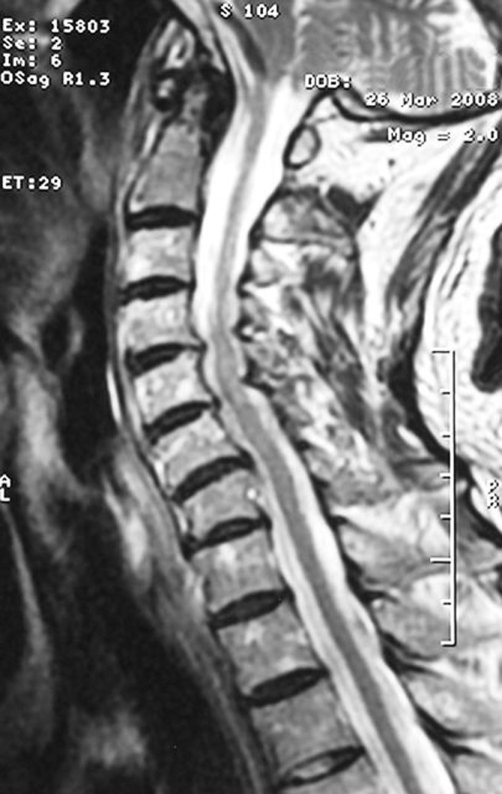
Case presentation: The case of an 85-year-old patient with a long history of neck pain caused by known multi-level cervical spine degeneration is presented. As conservative treatment became ineffective, he was sent for surgery. Pain character had changed from mechanical to nonmechanical. Therefore, new cervical Magnetic resonance imaging was requested, showing unexpected odontoid process osteolysis. Unknown lung cancer with adrenal and pancreatic metastases was revealed by further investigations.
Conclusion: Detailed pain characterization can already indicate the correct diagnosis. In case of new onset cervical neck pain, magnetic resonance imaging should be performed soon, if pain is characterized as nonmechanical.
Figures


Similar articles
-
Acute neck pain caused by atlanto-axial instability secondary to pathologic fracture involving odontoid process and C2 vertebral body: treatment with radiofrequency thermoablation, cement augmentation and odontoid screw fixation.Arch Orthop Trauma Surg. 2015 Sep;135(9):1211-5. doi: 10.1007/s00402-015-2266-y. Epub 2015 Jun 25. Arch Orthop Trauma Surg. 2015. PMID: 26109440
-
Clinical decision making associated with an undetected odontoid fracture in an older individual referred to physical therapy for the treatment of neck pain.J Orthop Sports Phys Ther. 2008 Jul;38(7):418-24. doi: 10.2519/jospt.2008.2687. Epub 2008 Jun 3. J Orthop Sports Phys Ther. 2008. PMID: 18591762
-
Lung Adenocarcinoma Presenting as Worsening of Chronic Neck Pain-A Cautionary Tale.Clin Med Insights Case Rep. 2017 Feb 10;10:1179547617691040. doi: 10.1177/1179547617691040. eCollection 2017. Clin Med Insights Case Rep. 2017. PMID: 28469500 Free PMC article.
-
Surgical treatment of chronic C1-C2 dislocation with absence of odontoid process using C1 hooks with C2 pedicle screws: a case report and review of literature.Spine (Phila Pa 1976). 2011 Aug 15;36(18):E1245-9. doi: 10.1097/BRS.0b013e318205620a. Spine (Phila Pa 1976). 2011. PMID: 21358484 Review.
-
Healing of type II odontoid fracture without surgery in an octogenarian - Case report and literature review.J Clin Neurosci. 2019 Jun;64:23-24. doi: 10.1016/j.jocn.2019.03.049. Epub 2019 Mar 30. J Clin Neurosci. 2019. PMID: 30940454 Review.
Cited by
-
Spastic quadriparesis due to pathological fracture of odontoid secondary to carcinoma prostate: A rare presentation.J Craniovertebr Junction Spine. 2017 Apr-Jun;8(2):153-155. doi: 10.4103/0974-8237.208045. J Craniovertebr Junction Spine. 2017. PMID: 28694601 Free PMC article.
References
-
- Aydinli U, Ozturk C, Bayram S, Sarihan S, Evrensel T, Yilmaz HS. Evaluation of lung cancer metastases to the spine. Acta Orthop Belg. 2006;2:592–597. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
