

Isolated long thoracic nerve paralysis - a rare complication of anterior spinal surgery: a case report
- PMID: 19830192
- PMCID: PMC2726530
- DOI: 10.4076/1752-1947-3-7366
Isolated long thoracic nerve paralysis - a rare complication of anterior spinal surgery: a case report
Abstract
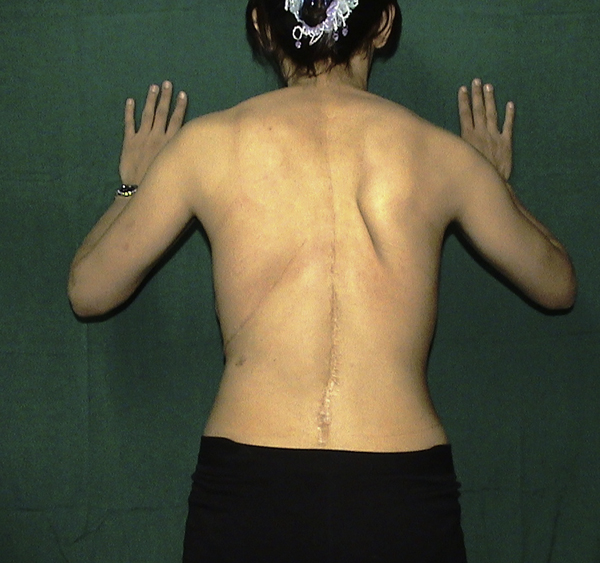
Introduction: Isolated long thoracic nerve injury causes paralysis of the serratus anterior muscle. Patients with serratus anterior palsy may present with periscapular pain, weakness, limitation of shoulder elevation and scapular winging.
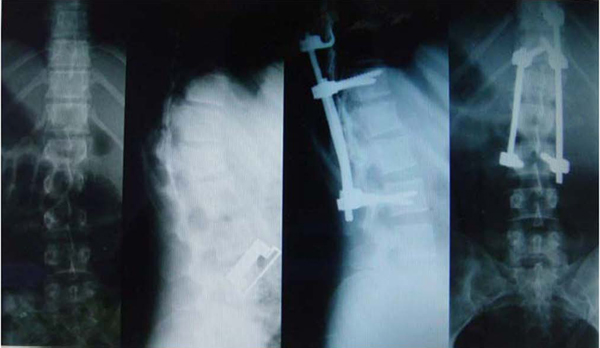
Case presentation: We present the case of a 23-year-old woman who sustained isolated long thoracic nerve palsy during anterior spinal surgery which caused external compressive force on the nerve.
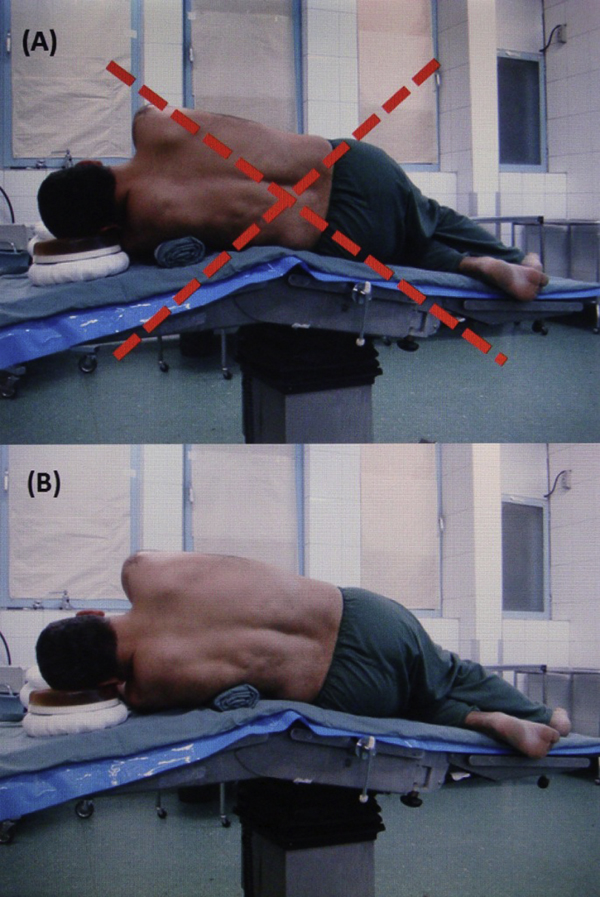
Conclusion: During positioning of patients into the lateral decubitus position, the course of the long thoracic nerve must be attended to carefully and the nerve should be protected from any external pressure.
Figures


Similar articles
-
Neurolysis of the Long Thoracic Nerve for Scapular Winging due to Isolated Serratus Anterior Palsy: Early and Midterm Results in 29 Patients.J Hand Microsurg. 2024 May 14;16(2):100031. doi: 10.1055/s-0043-1768478. eCollection 2024 Jun. J Hand Microsurg. 2024. PMID: 38855528 Free PMC article.
-
Scapular Winging Secondary to Apparent Long Thoracic Nerve Palsy in a Young Female Swimmer.J Brachial Plex Peripher Nerve Inj. 2015 Nov 6;10(1):e57-e61. doi: 10.1055/s-0035-1567806. eCollection 2015 Dec. J Brachial Plex Peripher Nerve Inj. 2015. PMID: 27917241 Free PMC article.
-
Scapular Winging Caused by Combined Palsy of the Spinal Accessory Nerve and the Long Thoracic Nerve: A Case Report.JBJS Case Connect. 2017 Apr-Jun;7(2):e23. doi: 10.2106/JBJS.CC.16.00162. JBJS Case Connect. 2017. PMID: 29244663
-
Anatomy, Etiology, and Management of Scapular Winging.J Hand Surg Am. 2019 Apr;44(4):321-330. doi: 10.1016/j.jhsa.2018.08.008. Epub 2018 Oct 3. J Hand Surg Am. 2019. PMID: 30292717 Review.
-
Long thoracic nerve injury.Clin Orthop Relat Res. 1999 Nov;(368):17-27. Clin Orthop Relat Res. 1999. PMID: 10613149 Review.
Cited by
-
Static winging of the scapula caused by osteochondroma in adults: a case series.J Med Case Rep. 2012 Oct 25;6:363. doi: 10.1186/1752-1947-6-363. J Med Case Rep. 2012. PMID: 23098161 Free PMC article.
-
Iatrogenic long thoracic nerve injury and scapular winging in posterior spinal fusion surgery: A case report.Clin Case Rep. 2022 Apr 26;10(4):e05746. doi: 10.1002/ccr3.5746. eCollection 2022 Apr. Clin Case Rep. 2022. PMID: 35498343 Free PMC article.
-
Long thoracic nerve injury in breast cancer patients treated with axillary lymph node dissection.Support Care Cancer. 2015 Jan;23(1):169-75. doi: 10.1007/s00520-014-2338-5. Epub 2014 Jul 18. Support Care Cancer. 2015. PMID: 25035064
References
LinkOut - more resources
Full Text Sources
