

Review
doi: 10.1007/s00383-009-2502-z.
Epub 2009 Oct 15.
Bowel management for the treatment of pediatric fecal incontinence
Affiliations
- PMID: 19830436
- PMCID: PMC2777229
- DOI: 10.1007/s00383-009-2502-z
Item in Clipboard
Review
Bowel management for the treatment of pediatric fecal incontinence
Pediatr Surg Int.
2009 Dec.
Abstract
Fecal incontinence is a devastating underestimated problem, affecting a large number of individuals all over the world. Most of the available literature relates to the management of adults. The treatments proposed are not uniformly successful and have little application in the pediatric population. This paper presents the experience of 30 years, implementing a bowel management program, for the treatment of fecal incontinence in over 700 pediatric patients, with a success rate of 95%. The main characteristics of the program include the identification of the characteristics of the colon of each patient; finding the specific type of enema that will clean that colon and the radiological monitoring of the process.
Figures

Contrast enema showing a dilated rectosigmoid

Contrast enema showing a non-dilated colon

Destroyed anal canal after a Hirschsprung’s disease operation. a External appearance (patulous anus). b Anal examination shows colonic mucosa anastomosed to skin (no pectinate line)

Redundant non-dilated colon of patients with spina bifida

Contrast enema showing a spastic rectosigmoid, after prolonged use of a phosphate-based enema
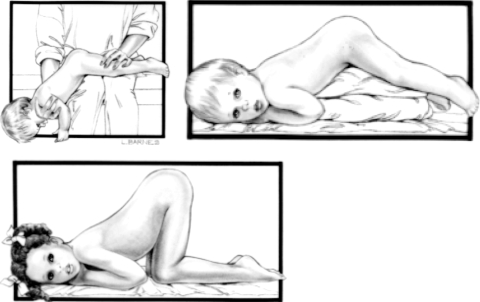
Child’s position to receive an enema according to their ages. Reprinted from Peña A, Levitt MA (2005) Pediatric surgical problems. In: Corman ML (ed) Colon and rectal surgery with kind permission from Lippincott Williams and Wilkins
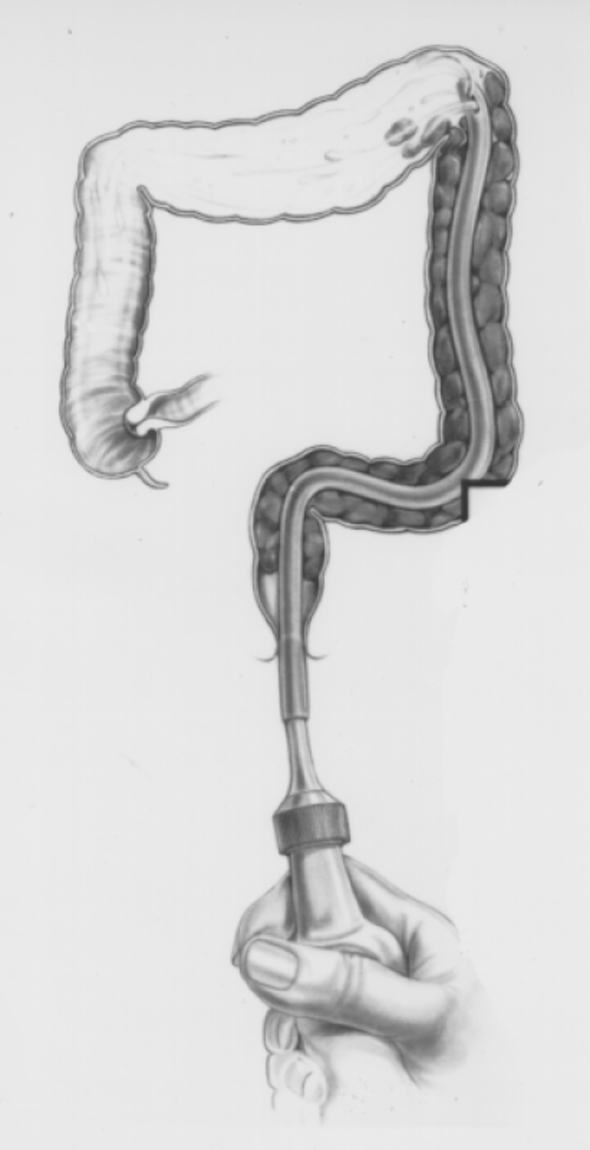
Enema technique showing the tube high in the left colon

Enema technique showing the Foley balloon inflated. Reprinted with kind permission from Ref. [38]

Abdominal radiograph showing stool in the rectum and descending colon

Abdominal radiograph showing a completely clean colon
References
-
- US census bureau http://www.census.gov/
-
- Peña A, Levitt MA (2005) Imperforate anus and cloacal malformations. In: Ashcraft KW, Holcomb GW, Murphy JP (eds) Pediatric surgery, 4th edn. W.B. Saunders, Philadelphia, pp 496–517
-
- Lary JM, Edmonds LD (1996) Prevalence of spina bifida at birth—United States, 1983–1990: a comparison of two surveillance systems. MMWR CDC Surveill 45:15–26 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
