

Scoring system for renal pathology in Fabry disease: report of the International Study Group of Fabry Nephropathy (ISGFN)
- PMID: 19833663
- PMCID: PMC2902894
- DOI: 10.1093/ndt/gfp528
Scoring system for renal pathology in Fabry disease: report of the International Study Group of Fabry Nephropathy (ISGFN)
Abstract
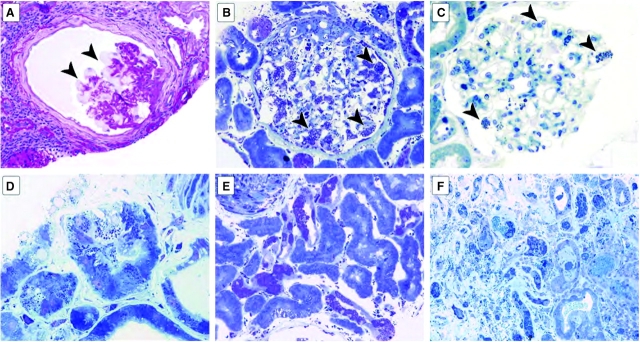
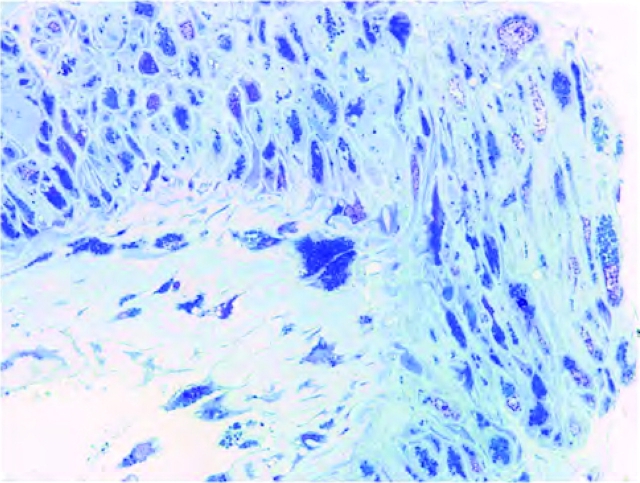
Background: In Fabry nephropathy, alpha-galactosidase deficiency leads to accumulation of glycosphingolipids in all kidney cell types, proteinuria and progressive loss of kidney function.
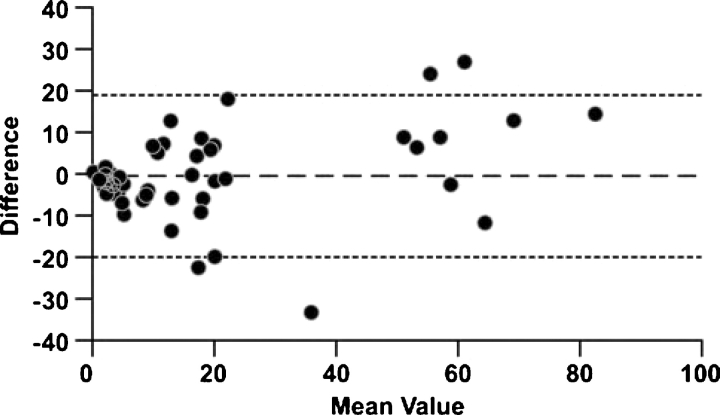
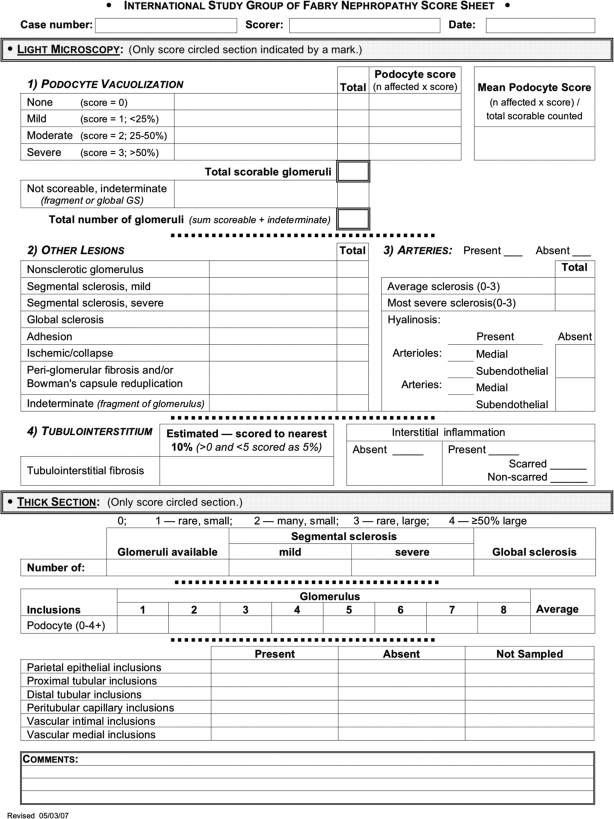
Methods: An international working group of nephrologists from 11 Fabry centres identified adult Fabry patients, and pathologists scored histologic changes on renal biopsies. A standardized scoring system was developed with a modified Delphi technique assessing 59 Fabry nephropathy cases. Each case was scored independently of clinical information by at least three pathologists with an average final score reported.
Results: We assessed 35 males (mean age 36.4 years) and 24 females (43.9 years) who mostly had clinically mild Fabry nephropathy. The average serum creatinine was 1.3 mg/dl (114.9 micromol/l); estimated glomerular filtration rate was 81.7 ml/min/1.73 m(2) and urine protein to creatinine ratio was 1.08 g/g (122.0 mg/mmol). Males had greater podocyte vacuolization on light microscopy (mean score) and glycosphingolipid inclusions on semi-thin sections than females. Males also had significantly more proximal tubule, peritubular capillary and vascular intimal inclusions. Arteriolar hyalinosis was similar, but females had significantly more arterial hyalinosis. Chronic kidney disease stage correlated with arterial and glomerular sclerosis scores. Significant changes, including segmental and global sclerosis, and interstitial fibrosis were seen even in patients with stage 1-2 chronic kidney disease with minimal proteinuria.
Conclusions: The development of a standardized scoring system of both disease-specific lesions, i.e. lipid deposition related, and general lesions of progression, i.e. fibrosis and sclerosis, showed a spectrum of histologic appearances even in early clinical stage of Fabry nephropathy. These findings support the role of kidney biopsy in the baseline evaluation of Fabry nephropathy, even with mild clinical disease. The scoring system will be useful for longitudinal assessment of prognosis and responses to therapy for Fabry nephropathy.
Figures
References
-
- Desnick R, Ioannou Y, Eng C. Alpha-galactosidase A deficiency: Fabry disease. In: Scriver CR, Beaudet A, Sly WS, Valle D, editors. The Metabolic and Molecular Bases of Inherited Disease. New York: McGraw-Hill; 2001. pp. 3733–3774.
-
- Branton MH, Schiffmann R, Sabnis SG, et al. Natural history of Fabry renal disease: influence of alpha-galactosidase A activity and genetic mutations on clinical course. Medicine (Baltimore) 2002;81:122–138. - PubMed
-
- Eng CM, Guffon N, Wilcox WR, et al. Safety and efficacy of recombinant human alpha-galactosidase A—replacement therapy in Fabry's disease. N Engl J Med. 2001;345:9–16. - PubMed
-
- Thurberg BL, Rennke H, Colvin RB, et al. Globotriaosylceramide accumulation in the Fabry kidney is cleared from multiple cell types after enzyme replacement therapy. Kidney Int. 2002;62:1933–1946. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
