

Coronary calcification in patients with chronic kidney disease and coronary artery disease
- PMID: 19833908
- PMCID: PMC2798876
- DOI: 10.2215/CJN.04320709
Coronary calcification in patients with chronic kidney disease and coronary artery disease
Abstract
Background and objectives: A close linkage between chronic kidney disease (CKD) and cardiovascular disease (CVD) has been demonstrated. Coronary artery calcification (CAC) is considered to be the causal link connecting them. The aim of the study is to determine the relationship between level of kidney function and the prevalence of CAC.
Design, setting, participants, & measurements: Autopsy subjects known to have coronary artery disease and a wide range of kidney function were studied. Patients without CKD were classified into five groups depending on estimated GFR (eGFR) and proteinuria: eGFR > or =60 ml/min/1.73 m(2) without proteinuria; CKD1/2: eGFR > or =60 ml/min/1.73 m(2) with proteinuria; CKD3: 60 ml/min/1.73 m(2) >eGFR > or =30 ml/min/1.73 m(2); CKD4/5: eGFR <30 ml/min/1.73 m(2); and CKD5D: on hemodialysis. Intimal and medial calcification of the coronary arteries was evaluated. Risk factors for CVD and uremia were identified as relevant to CAC using logistic regression analysis.
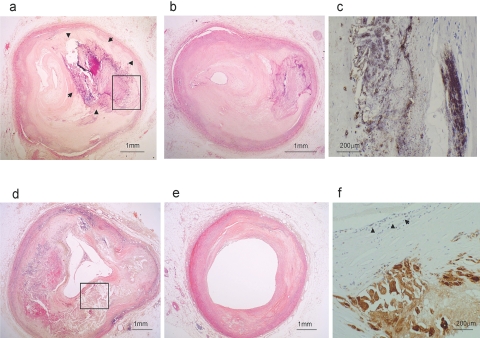
Results: Intimal calcification of plaques was present in all groups, but was most frequent and severe in the CKD5D group and less so in the CKD4/5 and CKD3 groups. Risk factors included luminal stenosis, age, smoking, diabetes, calcium-phosphorus product, inflammation, and kidney function. Medial calcification was seen in a small number of CKD4/5 and CKD5D groups. Risk factors were use of calcium-containing phosphate binders, hemodialysis treatment, and duration.
Conclusions: It was concluded that CAC was present in the intimal plaque of both nonrenal and renal patients. Renal function and traditional risks were linked to initimal calcification. Medial calcification occurred only in CKD patients.
Figures
Comment in
-
Coronary calcification in chronic kidney disease: morphology, mechanisms and mortality.Clin J Am Soc Nephrol. 2009 Dec;4(12):1883-5. doi: 10.2215/CJN.07611009. Epub 2009 Nov 19. Clin J Am Soc Nephrol. 2009. PMID: 19965543 No abstract available.
References
-
- US Renal Data System. Patient mortality and survival in ESRD. Am J Kidney Dis 34: S74–S86, 1999 - PubMed
-
- Nakai S, Masakane I, Akiba T, Shigematsu T, Yamagata K, Watanabe Y, Iseki K, Itami N, Shinoda T, Morozumi K, Shoji T, Marubayashi S, Morita O, Kimata N, Shoji T, Suzuki K, Tsuchida K, Nakamoto H, Hamano T, Yamashita A, Wakai K, Wada A, Tsubakihara Y: Overview of dialysis treatment in Japan as of 31 December 2006. Ther Apher Dial 12: 428–456, 2008 - PubMed
-
- Dzau VJ, Antman EM, Black HR, Hayes DL, Manson JE, Plutzky J, Popma JJ, Stevenson W: The cardiovascular disease continuum validated: Clinical evidence of improved patient outcomes. part II: Clinical trial evidence (acute coronary syndromes through renal disease) and future directions. Circulation 114: 2871–2891, 2006 - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresch J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey M, Pfeffer M, Raji L, Spinosa DJ, Wilson PW: American Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention: Kidney disease as a risk factor for development of cardiovascular diseases: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 108: 2154–2169, 2003 - PubMed
-
- Hostetter TH: Chronic kidney disease predicts cardiovascular disease. N Engl J Med 351: 1344–1346, 2004 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
