

The Li-Fraumeni syndrome (LFS): a model for the initiation of p53 signatures in the distal Fallopian tube
- PMID: 19834951
- PMCID: PMC2841524
- DOI: 10.1002/path.2624
The Li-Fraumeni syndrome (LFS): a model for the initiation of p53 signatures in the distal Fallopian tube
Abstract
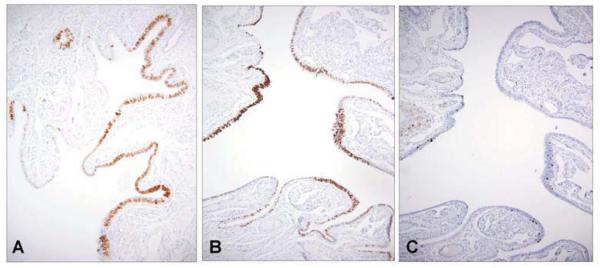
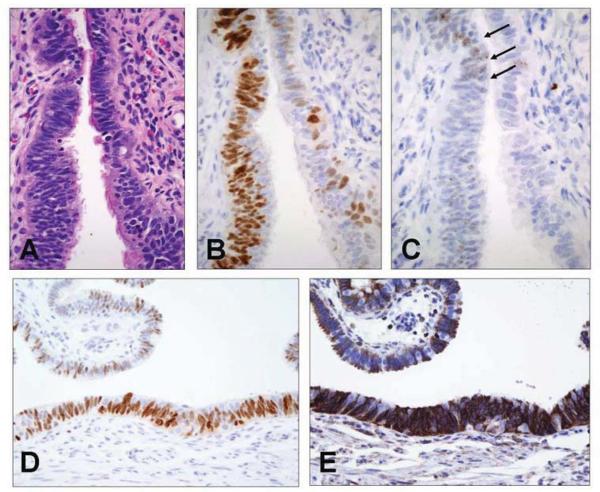
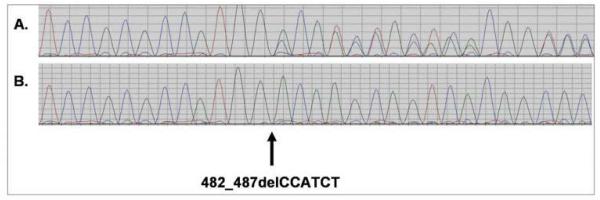
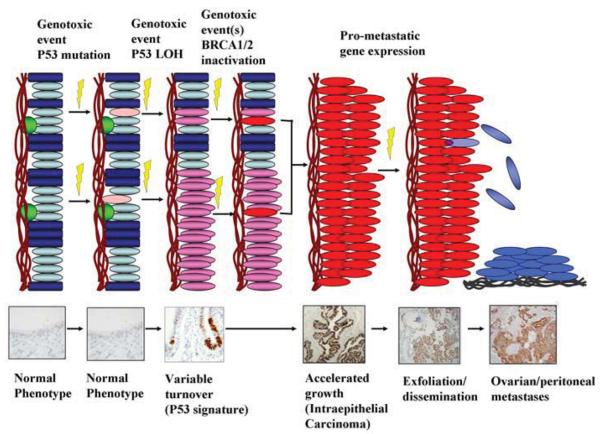
A candidate early precursor to pelvic serous cancer, the 'p53 signature', is commonly found in the benign mucosa of the distal Fallopian tube and harbours p53 mutations and evidence of DNA damage. We examined tubes from women with pre-existing (germ-line) mutations in p53 [Li-Fraumeni syndrome (LFS)] for evidence of this precursor. Fallopian tubes from two cases of LFS were immunostained for p53, Ki-67 (proliferation) and H2AX (DNA damage response) and analysed for p53 mutations by laser capture microdissection (LCM) and p53 genomic sequencing (exons 2-11). A common single nucleotide repeat (snp) in exon 3 (rs1042522) and deletion sequencing chromatograms in exon 4 were examined in combination to estimate LOH in both LFS tubes and advanced serous carcinomas from the general population. LFS tubal epithelium contained abundant (10-20 per section) p53 signatures with evidence of DNA damage and low proliferative activity. Six of 11 LFS microdissected p53 signatures (55%) and 15 of 21 serous carcinomas (71%) revealed LOH at the p53 locus, relative to background epithelium. The LFS model confirms prior observations that the distal Fallopian tube is particularly prone to focal epithelial p53 gene inactivation-p53 mutation and LOH-in the absence of malignancy or increased epithelial proliferation. The fact that the LFS is not associated with ovarian cancers is consistent with the concept that loss of p53 function must be accompanied by at least one more genotoxic event (including BRCA1/2 functional inactivation) to produce the malignant phenotype. This is in keeping with a general model of carcinogenesis, in which different and often independent risk factors operate at multiple points in the serous carcinogenic spectrum.
Figures
Comment in
-
The emerging role of the distal Fallopian tube and p53 in pelvic serous carcinogenesis.J Pathol. 2010 Jan;220(1):5-6. doi: 10.1002/path.2630. J Pathol. 2010. PMID: 19882674
References
-
- Shan W, Liu J. Epithelial ovarian cancer: focus on genetics and animal models. Cell Cycle. 2009;8:731–5. - PubMed
-
- Brewer MA, Mitchell MF, Bast RC. Prevention of ovarian cancer. In Vivo. 1999;13:99–106. - PubMed
-
- Bell DA, Scully RE. Early de novo ovarian carcinoma. A study of fourteen cases. Cancer. 1994;73:1859–64. - PubMed
-
- Piek JM, Kenemans P, Verheijen RH. Intraperitoneal serous adenocarcinoma: a critical appraisal of three hypotheses on its cause. Am J Obstet Gynecol. 2004;191:718–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
