

Late gastrointestinal toxicity after dose-escalated conformal radiotherapy for early prostate cancer: results from the UK Medical Research Council RT01 trial (ISRCTN47772397)
- PMID: 19836155
- PMCID: PMC2937212
- DOI: 10.1016/j.ijrobp.2009.05.052
Late gastrointestinal toxicity after dose-escalated conformal radiotherapy for early prostate cancer: results from the UK Medical Research Council RT01 trial (ISRCTN47772397)
Abstract
Purpose: In men with localized prostate cancer, dose-escalated conformal radiotherapy (CFRT) improves efficacy outcomes at the cost of increased toxicity. We present a detailed analysis to provide further information about the incidence and prevalence of late gastrointestinal side effects.
Methods and materials: The UK Medical Research Council RT01 trial included 843 men with localized prostate cancer, who were treated for 6 months with neoadjuvant radiotherapy and were randomly assigned to either 64-Gy or 74-Gy CFRT. Toxicity was evaluated before CFRT and during long-term follow-up using Radiation Therapy Oncology Group (RTOG) grading, the Late Effects on Normal Tissue: Subjective, Objective, Management (LENT/SOM) scale, and Royal Marsden Hospital assessment scores. Patients regularly completed Functional Assessment of Cancer Therapy--Prostate (FACT-P) and University of California, Los Angeles, Prostate Cancer Index (UCLA-PCI) questionnaires.
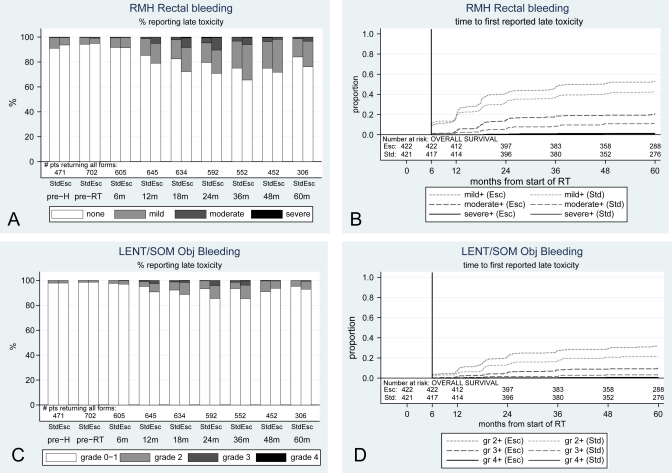
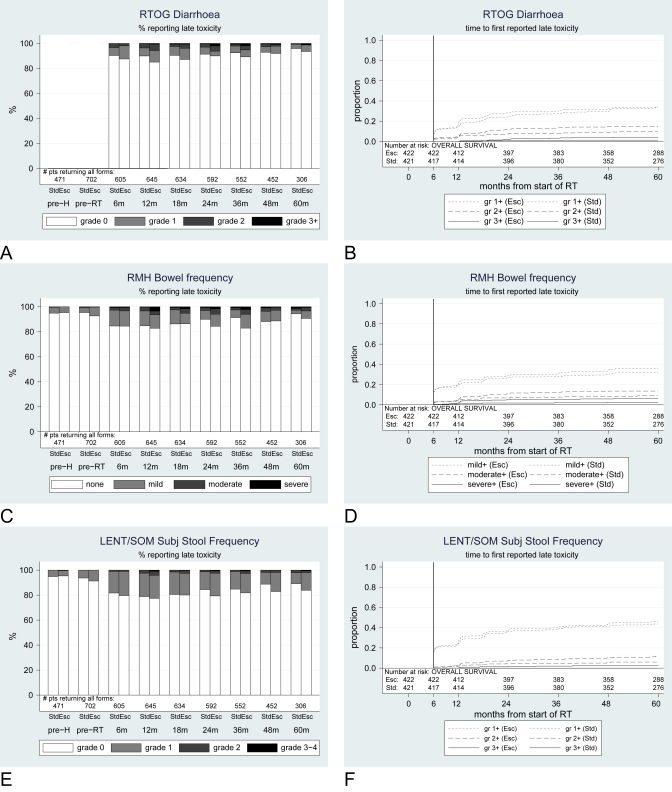
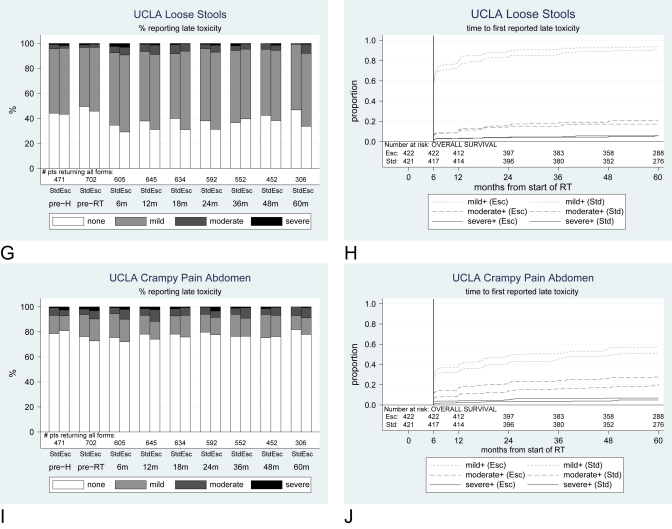
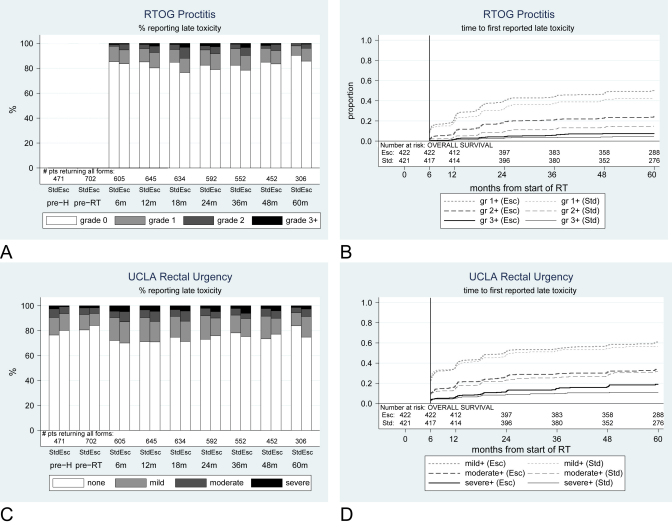
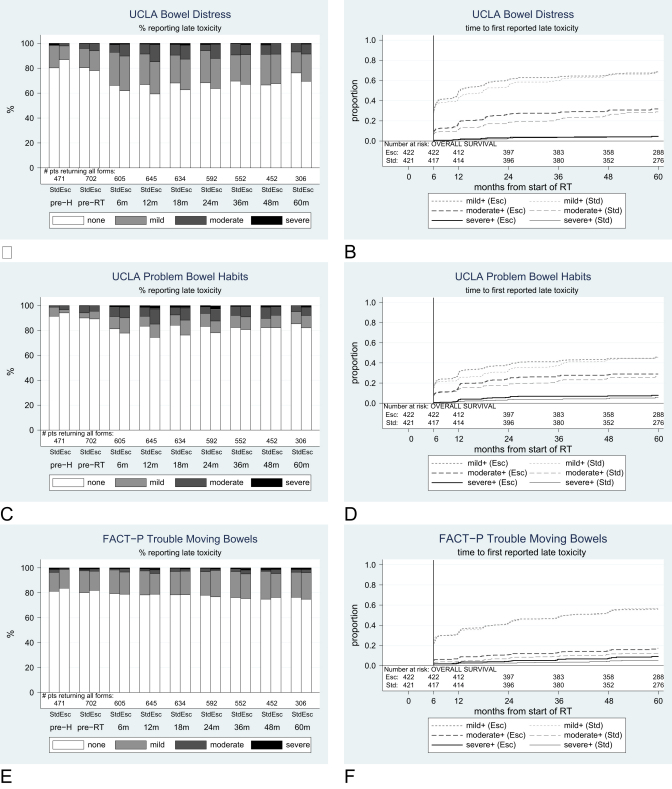
Results: In the dose-escalated group, the hazard ratio (HR) for rectal bleeding (LENT/SOM grade >or=2) was 1.55 (95% CI, 1.17-2.04); for diarrhea (LENT/SOM grade >or=2), the HR was 1.79 (95% CI, 1.10-2.94); and for proctitis (RTOG grade >or=2), the HR was 1.64 (95% CI, 1.20-2.25). Compared to baseline scores, the prevalence of moderate and severe toxicities generally increased up to 3 years and than lessened. At 5 years, the cumulative incidence of patient-reported severe bowel problems was 6% vs. 8% (standard vs. escalated, respectively) and severe distress was 4% vs. 5%, respectively.
Conclusions: There is a statistically significant increased risk of various adverse gastrointestinal events with dose-escalated CFRT. This remains at clinically acceptable levels, and overall prevalence ultimately decreases with duration of follow-up.
(c) 2010. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kuban D.A., Tucker S.L., Dong L. Long-term results of the M.D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:67–74. - PubMed
-
- Peeters S.T.H., Heemsbergen W.D., Koper P.C. Dose response in radiotherapy for localized prostate cancer: Results of the Dutch multicenter phase III randomized trial comparing 68 Gy with 78 Gy. J Clin Oncol. 2006;24 1990–1906. - PubMed
-
- Al-Mamgani A., Van Putten W.L.J., Heemsbergen W.D. Update of Dutch multicenter dose-escalation trial of radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2008;72:980–988. - PubMed
-
- Zietman A.L., DeSilvio M.L., Slater J.D. Comparison of conventional-dose versus high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate. JAMA. 2005;294:1233–1239. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
