

Dose response and efficacy of spinal manipulation for chronic cervicogenic headache: a pilot randomized controlled trial
- PMID: 19837005
- PMCID: PMC2819630
- DOI: 10.1016/j.spinee.2009.09.002
Dose response and efficacy of spinal manipulation for chronic cervicogenic headache: a pilot randomized controlled trial
Abstract
Background context: Systematic reviews of randomized controlled trials suggest that spinal manipulative therapy (SMT) is efficacious for care of cervicogenic headache (CGH). The effect of SMT dose on outcomes has not been studied.
Purpose: To compare the efficacy of two doses of SMT and two doses of light massage (LM) for CGH.
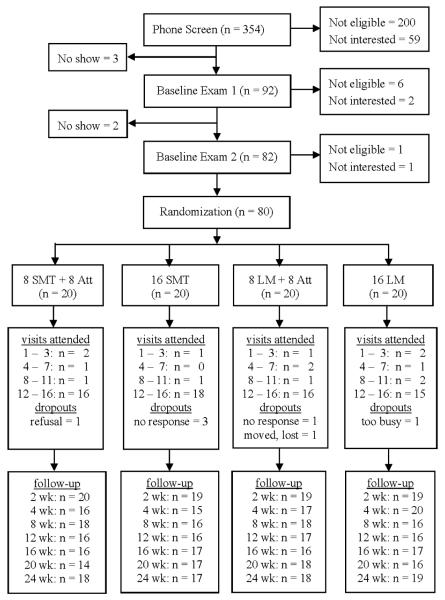
Patient sample: Eighty patients with chronic CGH.
Main outcome measures: Modified Von Korff pain and disability scales for CGH and neck pain (minimum clinically important difference=10 on 100-point scale), number of headaches in the last 4 weeks, and medication use. Data were collected every 4 weeks for 24 weeks. The primary outcome was the CGH pain scale.
Methods: Participants were randomized to either 8 or 16 treatment sessions with either SMT or a minimal LM control. Patients were treated once or twice per week for 8 weeks. Adjusted mean differences (AMD) between groups were computed using generalized estimating equations for the longitudinal outcomes over all follow-up time points (profile) and using regression modeling for individual time points with baseline characteristics as covariates and with imputed missing data.
Results: For the CGH pain scale, comparisons of 8 and 16 treatment sessions yielded small dose effects: |AMD|</=5.6. There was an advantage for SMT over the control: AMD=-8.1 (95% confidence interval=-13.3 to -2.8) for the profile, -10.3 (-18.5 to -2.1) at 12 weeks, and -9.8 (-18.7 to -1.0) at 24 weeks. For the higher dose patients, the advantage was greater: AMD=-11.9 (-19.3 to -4.6) for the profile, -14.2 (-25.8 to -2.6) at 12 weeks, and -14.4 (-26.9 to -2.0) at 24 weeks. Patients receiving SMT were also more likely to achieve a 50% improvement in pain scale: adjusted odds ratio=3.6 (1.6 to 8.1) for the profile, 3.1 (0.9 to 9.8) at 12 weeks, and 3.1 (0.9 to 10.3) at 24 weeks. Secondary outcomes showed similar trends favoring SMT. For SMT patients, the mean number of CGH was reduced by half.
Conclusions: Clinically important differences between SMT and a control intervention were observed favoring SMT. Dose effects tended to be small.
Copyright (c) 2010 Elsevier Inc. All rights reserved.
Figures


Comment in
-
Choosing a treatment for cervicogenic headache: when? what? how much?Spine J. 2010 Feb;10(2):169-71. doi: 10.1016/j.spinee.2009.10.013. Epub 2009 Dec 11. Spine J. 2010. PMID: 20004621 No abstract available.
-
Spinal manipulation for headache?Spine J. 2011 Jan;11(1):94; author reply 94-5. doi: 10.1016/j.spinee.2010.10.017. Spine J. 2011. PMID: 21168104 No abstract available.
References
-
- Rasmussen BK, Jensen R, Schroll M, Olesen J. Epidmiology of headache in a general population-a prevalence study. J Clin Epidemiol. 1991;44:1147–57. - PubMed
-
- Castillo J, Munoz P, Guitera V, Pascual J. Epidemiology of chronic daily headache in the general population. Headache. 1999;39:190–6. - PubMed
-
- Scher AI, Stewart WF, Liberman J, Lipton RB. Prevalence of frequent headache in a population sample. Headache. 1998;38:497–506. - PubMed
-
- Nilsson-Grunnet N. Epidemiology of Headache. Euro J Chiro. 2002;49:33–5.
-
- Solomon GD, Skobieranda FG, Gragg LA. Quality of life and well-being of headache patients: measurement by the Medical outcomes study instrument. Headache. 1993:351–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
