

Adaptive changes in autogenous vein grafts for arterial reconstruction: clinical implications
- PMID: 19837532
- PMCID: PMC2834835
- DOI: 10.1016/j.jvs.2009.07.102
Adaptive changes in autogenous vein grafts for arterial reconstruction: clinical implications
Abstract
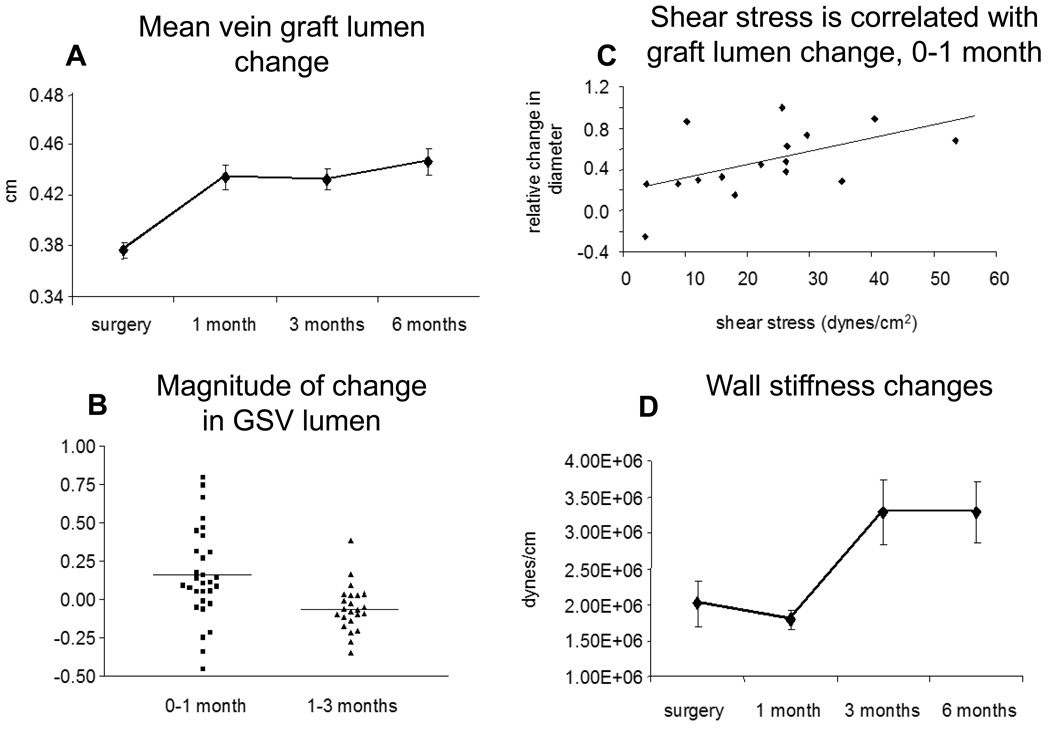
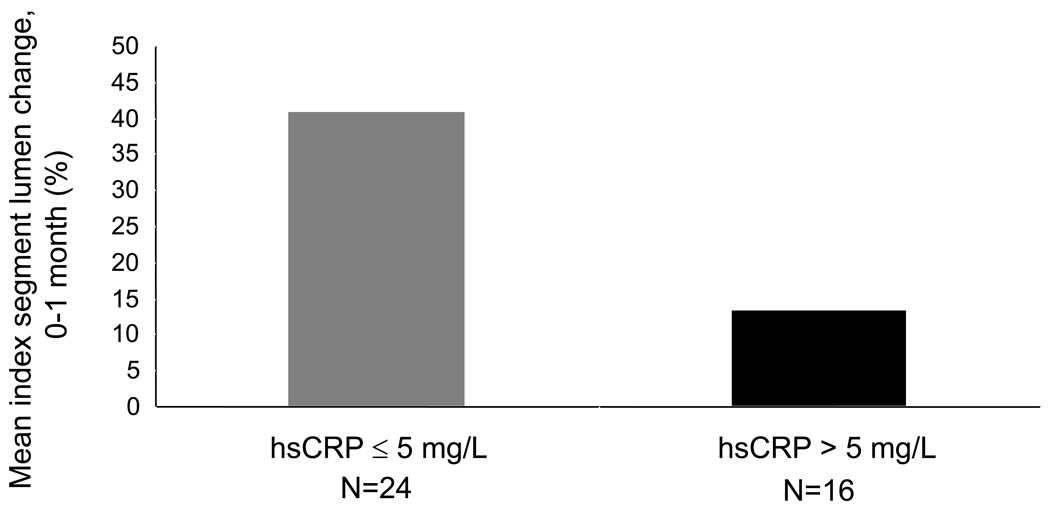
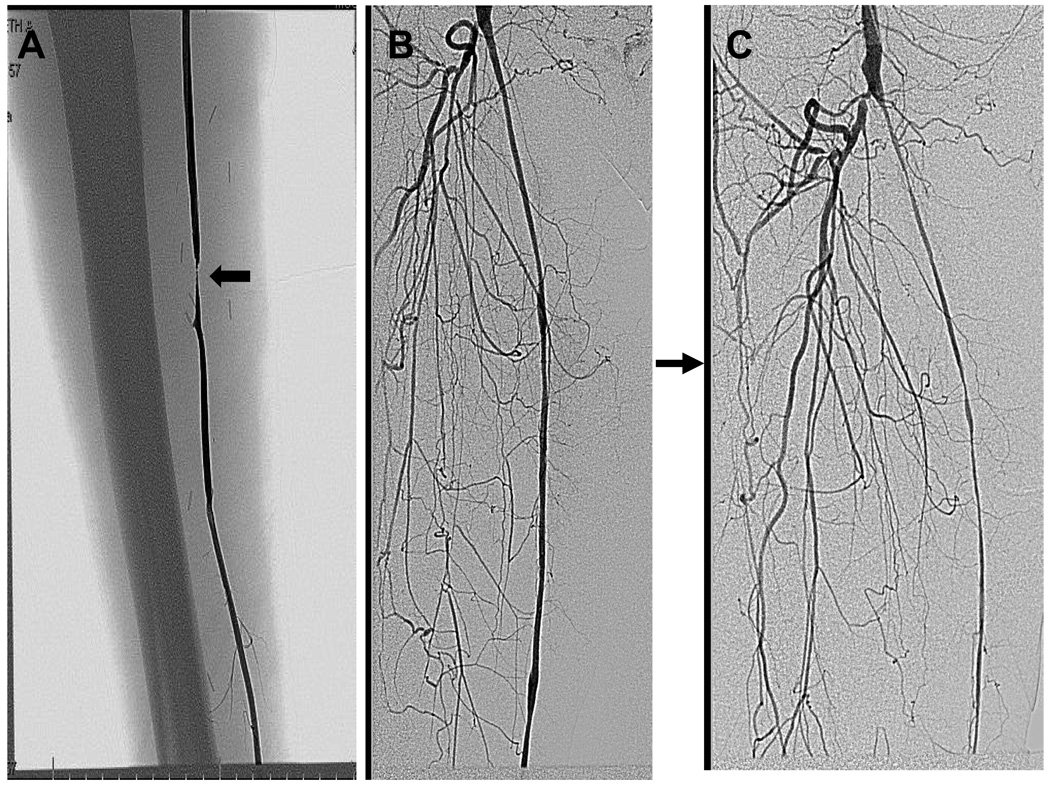
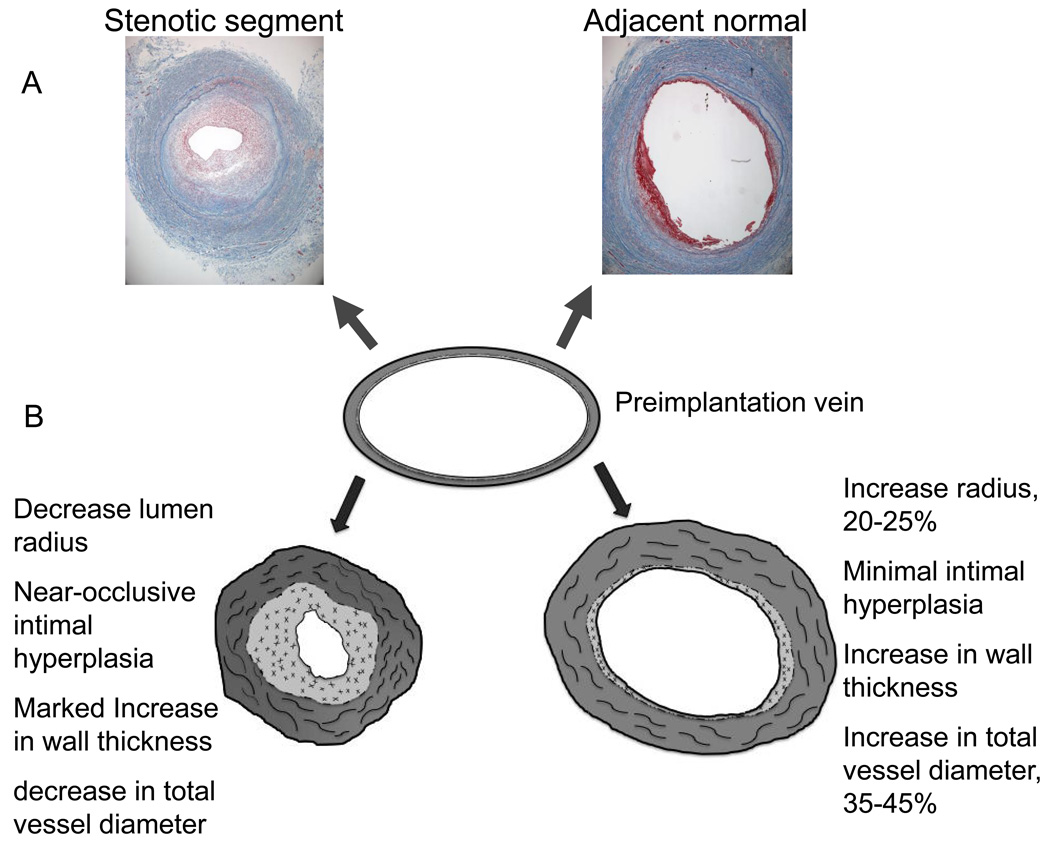
For patients with the most severe manifestations of lower extremity arterial occlusive disease, bypass surgery using autogenous vein has been the most durable reconstruction. However, the incidence of bypass graft stenosis and graft failure remains substantial and wholesale improvements in patency are lacking. One potential explanation is that stenosis arises not only from over exuberant intimal hyperplasia, but also due to insufficient adaptation or remodeling of the vein to the arterial environment. Although in vivo human studies are difficult to conduct, recent advances in imaging technology have made possible a more comprehensive structural examination of vein bypass maturation. This review summarizes recent translational efforts to understand the structural and functional properties of human vein grafts and places it within the context of the rich existing literature of vein graft failure.
Figures
References
-
- Rosamond W, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25–e146. - PubMed
-
- Hirsch AT, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. Jama. 2001;286(11):1317–1324. - PubMed
-
- Beckman JA, et al. Ascorbate restores endothelium-dependent vasodilation impaired by acute hyperglycemia in humans. Circulation. 2001;103(12):1618–1623. - PubMed
-
- Conte MS, et al. Genetic interventions for vein bypass graft disease: a review. J Vasc Surg. 2002;36(5):1040–1052. - PubMed
-
- Braun-Dullaeus RC, Mann MJ, Dzau VJ. Cell cycle progression: new therapeutic target for vascular proliferative disease. Circulation. 1998;98(1):82–89. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
