

Change in blood-brain barrier permeability during pediatric diabetic ketoacidosis treatment
- PMID: 19838141
- PMCID: PMC2913885
- DOI: 10.1097/PCC.0b013e3181c013f4
Change in blood-brain barrier permeability during pediatric diabetic ketoacidosis treatment
Abstract
Objective: Cerebral edema is a devastating complication of pediatric diabetic ketoacidosis. We aimed to examine blood-brain barrier permeability during treatment of diabetic ketoacidosis in children.
Design: Prospective observational study.
Setting: Seattle Children's Hospital, Seattle, WA.
Patients: Children admitted with diabetic ketoacidosis (pH <7.3, HCO3 <15 mEq/L, glucose >300 mg/dL, and ketosis).
Interventions: None.
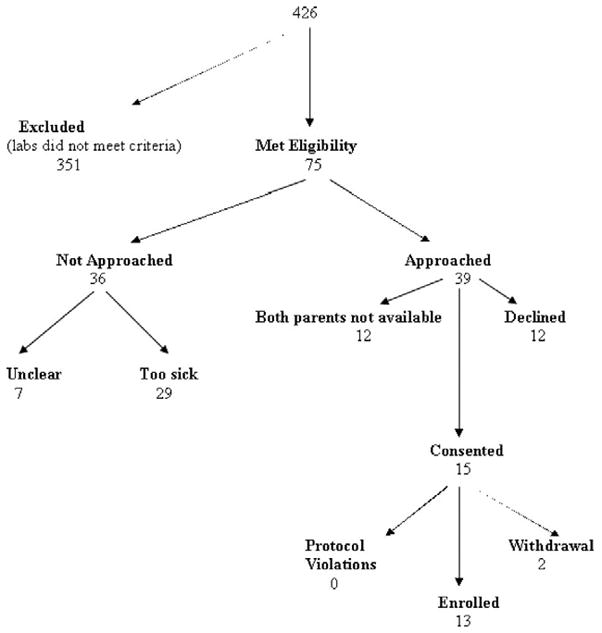
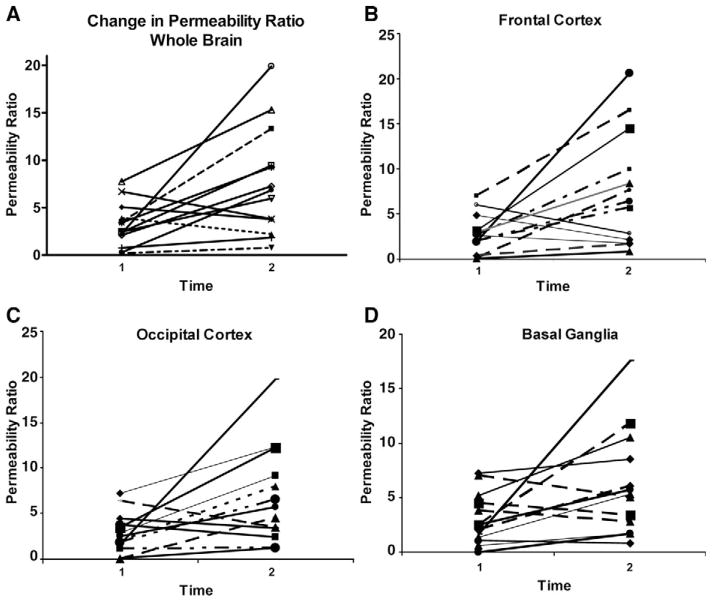
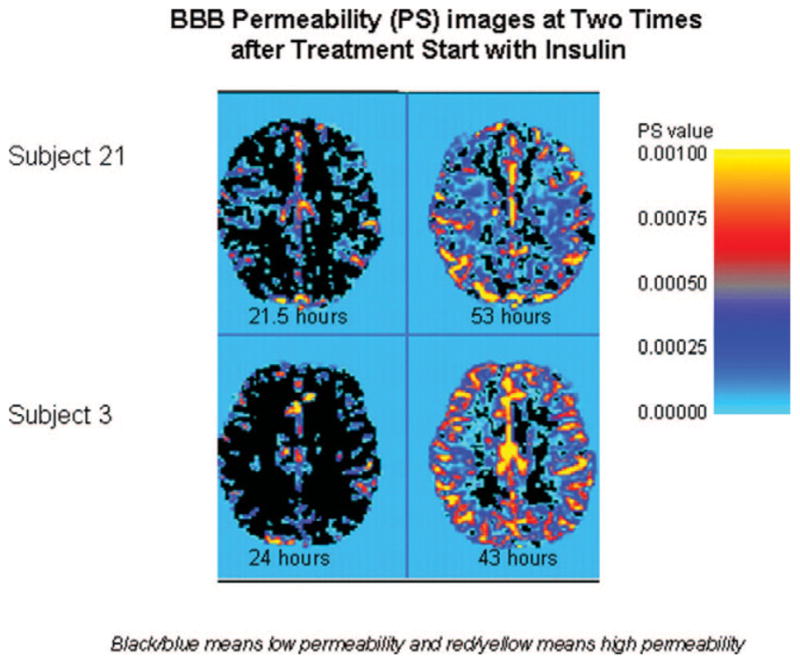
Measurements and main results: Subjects underwent two serial paired contrast-enhanced perfusion (gadolinium) and diffusion magnetic resonance imaging scans. Change in whole brain and regional blood-brain barrier permeability (permeability ratio*100 and % permeability ratio change) between illness and recovery were determined. Time 0 reflects start of insulin treatment. Thirteen children (median age 10.0 +/- 1.1 yrs; seven female) with diabetic ketoacidosis were enrolled. Permeability ratio increased from time 1 (first magnetic resonance image after time 0) to time 2 (second magnetic resonance image after time 0) in the frontal cortex (ten of 13 subjects), occipital cortex (ten of 13 subjects), and basal ganglia (nine of 13). Whole brain permeability ratio increased from time 1 to time 2 (160%) and regional increase in permeability ratio was greatest in the frontal cortex (148%) compared with the occipital cortex (128%) and basal ganglia (112%).
Conclusions: Overall, whole brain and regional blood-brain barrier permeability increased in most subjects during diabetic ketoacidosis treatment. The frontal region had more blood-brain barrier permeability than other brain regions examined.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Understanding the pathophysiology of cerebral edema in diabetic ketoacidosis: another brick in the wall?Pediatr Crit Care Med. 2010 May;11(3):421-3. doi: 10.1097/PCC.0b013e3181d4f70c. Pediatr Crit Care Med. 2010. PMID: 20453613 No abstract available.
References
-
- Rewers A, Klingensmith G, Davis C, et al. Presence of diabetic ketoacidosis at diagnosis of diabetes mellitus in youth: the Search for Diabetes in Youth Study. Pediatrics. 2008;121:e1258–e1266. - PubMed
-
- Rewers A, Chase HP, Mackenzie T, et al. Predictors of acute complications in children with type 1 diabetes. JAMA. 2002;287:2511–2518. - PubMed
-
- Hanas R, Lindblad B, Lindgren F. Diabetic ketoacidosis and cerebral edema in Sweden, a 2-year population study. Abstr Diabetes. 2004;53(Suppl 2):A421. - PubMed
-
- Roche EF, Menon A, Gill D, et al. Clinical presentation of type 1 diabetes. Pediatr Diabetes. 2005;6:75–78. - PubMed
-
- Edge JA. Cerebral oedema during treatment of diabetic ketoacidosis: Are we any nearer finding a cause? Diabetes Metab Res Rev. 2000;16:316–324. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
