

Circulating mesothelin protein and cellular antimesothelin immunity in patients with pancreatic cancer
- PMID: 19843662
- PMCID: PMC2782601
- DOI: 10.1158/1078-0432.CCR-09-0565
Circulating mesothelin protein and cellular antimesothelin immunity in patients with pancreatic cancer
Abstract
Purpose: Mesothelin is a glycoprotein expressed on normal mesothelial cells and is overexpressed in several histologic types of tumors including pancreatic adenocarcinomas. A soluble form of mesothelin has been detected in patients with ovarian cancer and malignant mesothelioma, and has prognostic value. Mesothelin has also been considered as a target for immune-based therapies. We conducted a study on the potential clinical utility of mesothelin as a biomarker for pancreatic disease and therapeutic target pancreatic cancer.
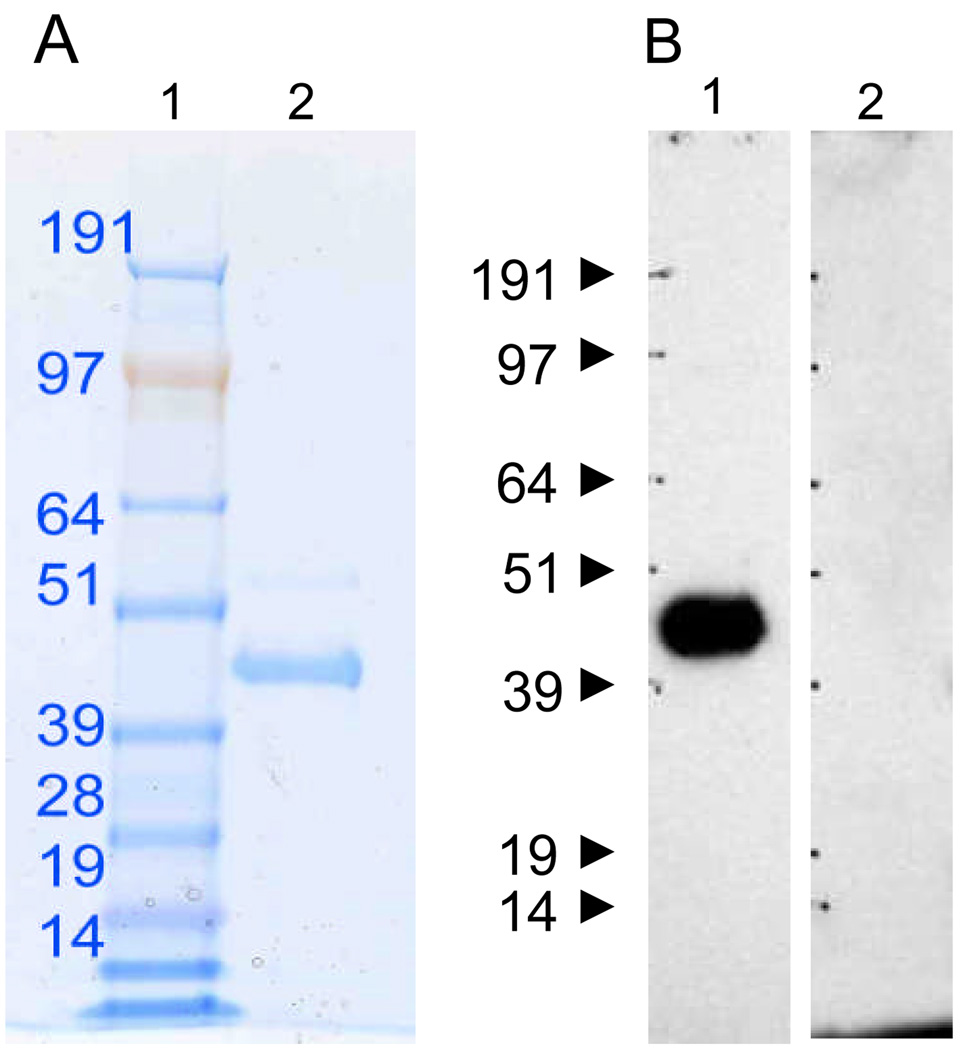
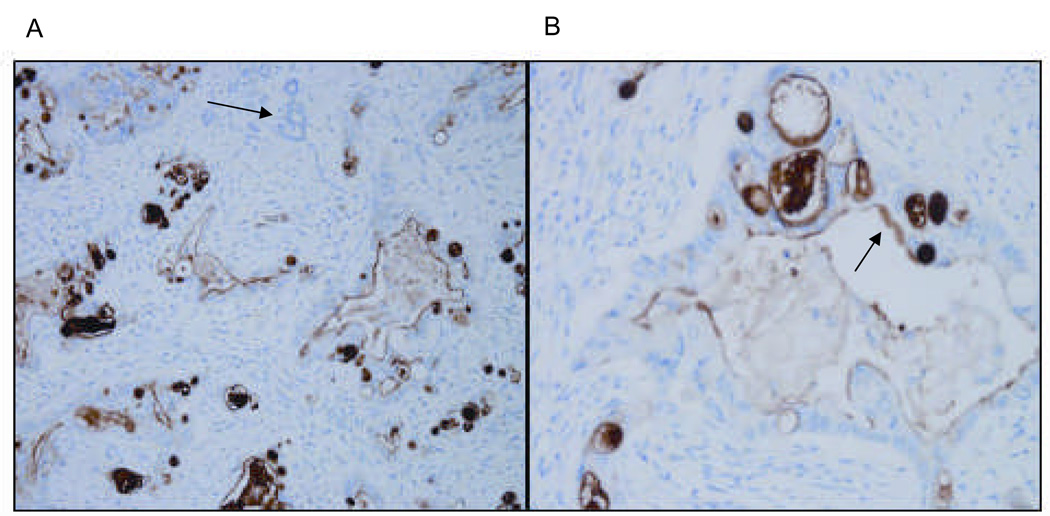
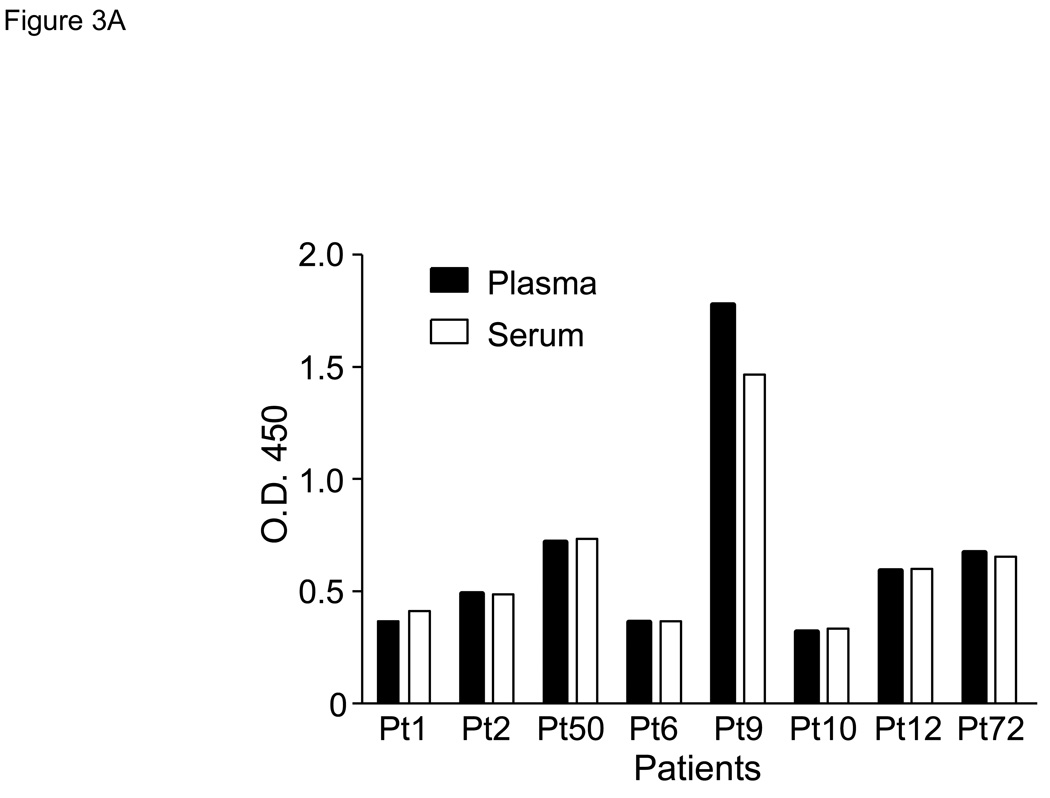
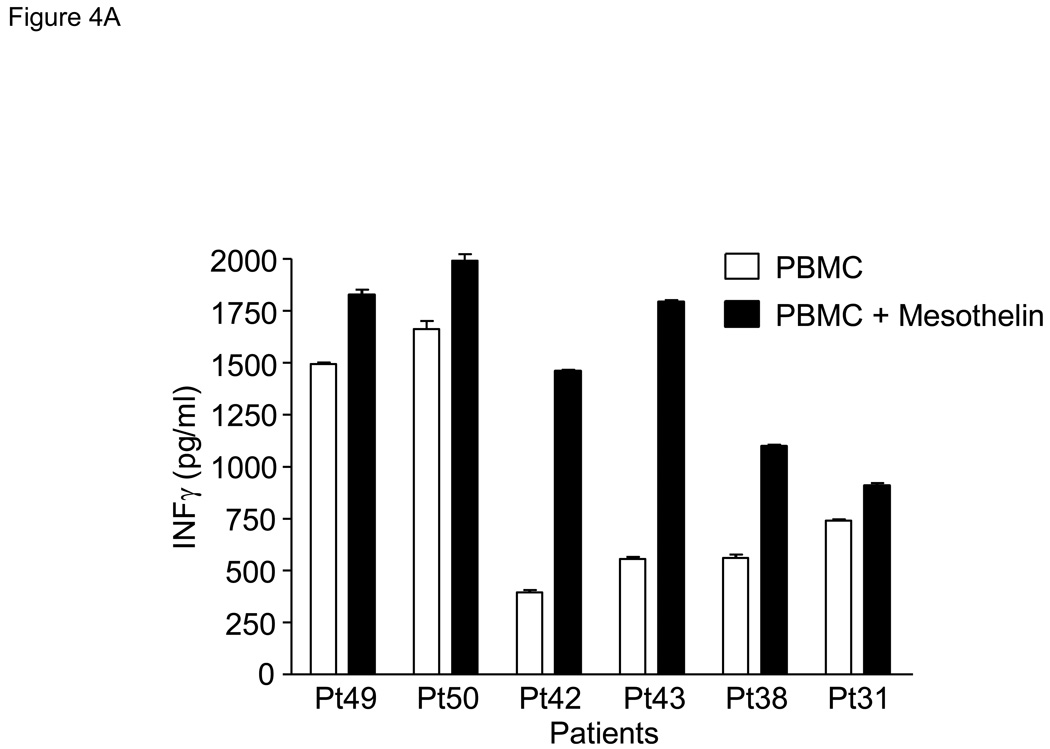
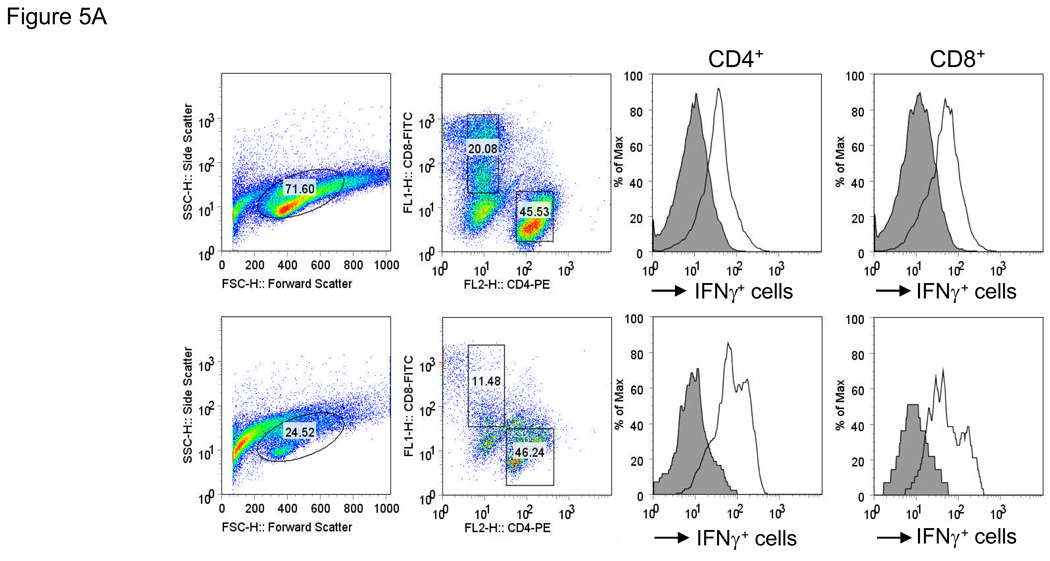
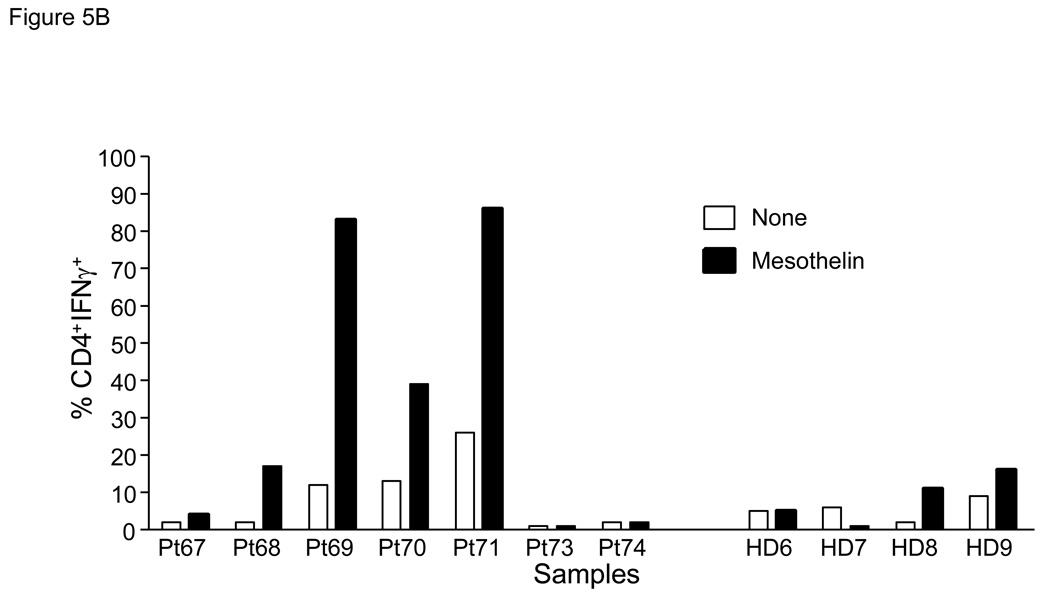
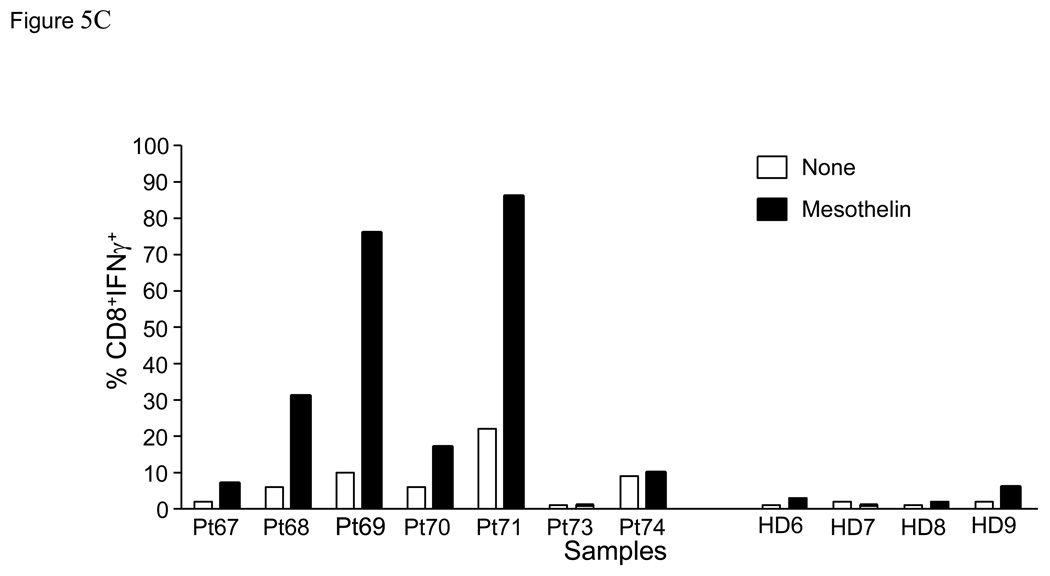
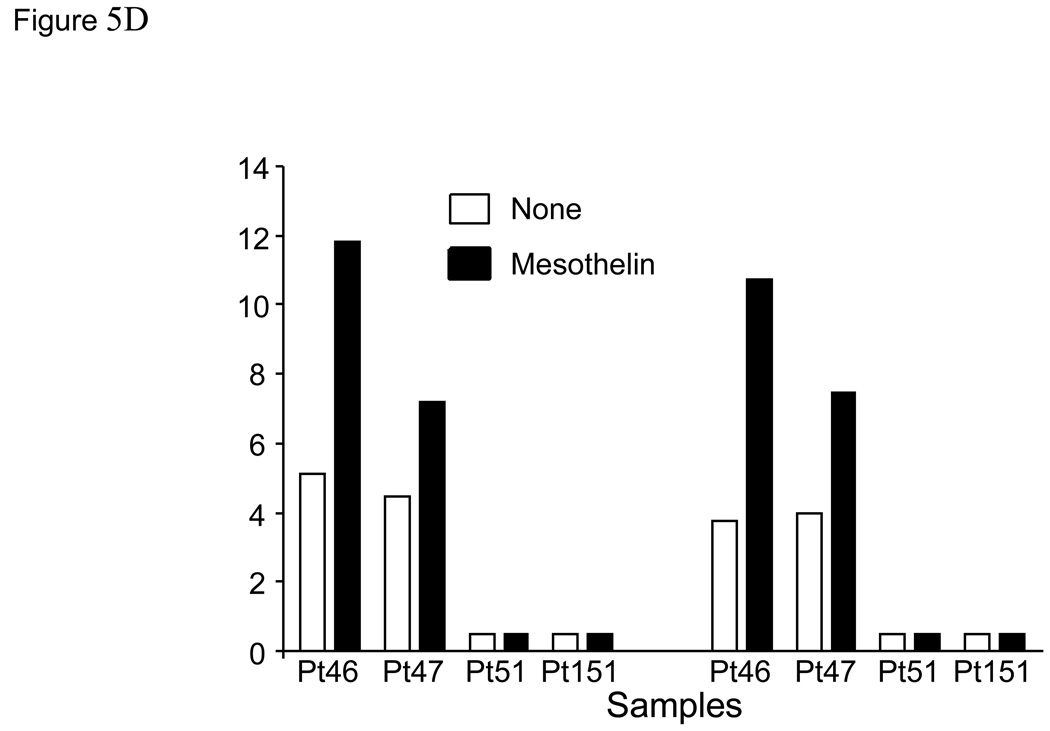
Experimental design: Tumor cell-bound and soluble mesothelin in patients was evaluated by immunohistochemistry and ELISA, respectively. The in vitro cellular immune response to mesothelin was evaluated by INF gamma ELISA and intracellular cytokine staining for IFN gamma in CD4(+) and CD8(+) T cells. The level of circulating antibodies to mesothelin was measured by ELISA.
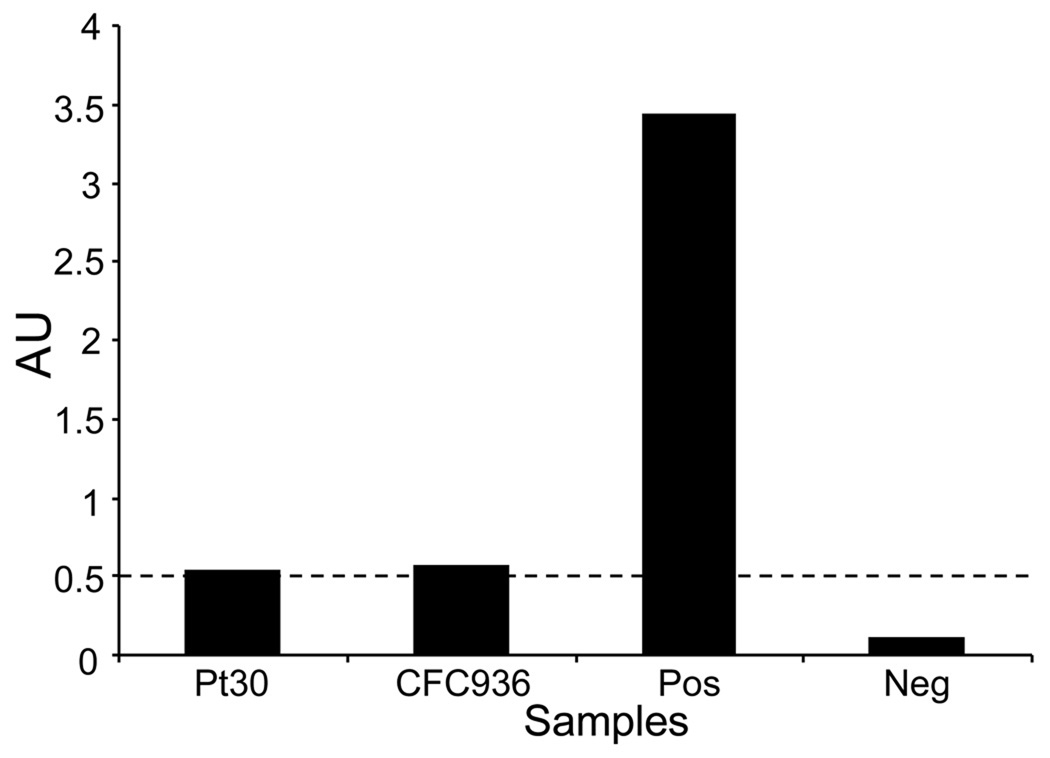
Results: All tumor tissue from patients with pancreatic adenocarcinoma expressed mesothelin (n = 10). Circulating mesothelin protein was detected in patients with pancreatic adenocarcinoma (73 of 74 patients) and benign pancreatic disease (5 of 5) but not in healthy individuals. Mesothelin-specific CD4(+) and CD8(+) T cells were generated from peripheral blood lymphocytes of patients with pancreatic cancer in 50% of patients compared with only 20% of healthy individuals. Antibodies reactive to mesothelin were detected in <3% of either patients or healthy individuals.
Conclusions: Circulating mesothelin is a useful biomarker for pancreatic disease. Furthermore, mesothelin-specific T cells can be induced in patients with pancreatic cancer. This suggests that mesothelin is a potential target for immune-based intervention strategies in pancreatic cancer.
Figures


References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J.Clin. 2008;58:71–96. - PubMed
-
- Kubuschok B, Neumann F, Breit R, Sester M, Schormann C, Wagner C, et al. Naturally occurring T-cell response against mutated p21 ras oncoprotein in pancreatic cancer. Clin.Cancer Res. 2006;12:1365–1372. - PubMed
-
- Schmitz-Winnenthal FH, Volk C, Z'graggen K, Galindo L, Nummer D, Ziouta Y, et al. High frequencies of functional tumor-reactive T cells in bone marrow and blood of pancreatic cancer patients. Cancer Res. 2005;65:10079–10087. - PubMed
-
- Schmitz-Winnenthal FH, Escobedo LV, Beckhove P, Schirrmacher V, Bucur M, Ziouta Y, et al. Specific immune recognition of pancreatic carcinoma by patient-derived CD4 and CD8 T cells and its improvement by interferon-gamma. Int.J.Oncol. 2006;28:1419–1428. - PubMed
-
- Fukunaga A, Miyamoto M, Cho Y, Murakami S, Kawarada Y, Oshikiri T, et al. CD8+ tumor-infiltrating lymphocytes together with CD4+ tumor-infiltrating lymphocytes and dendritic cells improve the prognosis of patients with pancreatic adenocarcinoma. Pancreas. 2004;28:e26–e31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
