

Diabetic bladder dysfunction: current translational knowledge
- PMID: 19846137
- PMCID: PMC4684267
- DOI: 10.1016/j.juro.2009.08.070
Diabetic bladder dysfunction: current translational knowledge
Abstract
Purpose: Diabetes mellitus, a metabolic disorder caused by an absolute or relative deficiency of insulin, is a debilitating and costly disease with multiple serious complications. Lower urinary tract complications are among the most common complications of diabetes mellitus. The most common, bothersome lower urinary tract complication of diabetes mellitus is diabetic cystopathy or diabetic bladder dysfunction. We reviewed the current translational knowledge of diabetic bladder dysfunction.
Materials and methods: We performed a search of the English literature through PubMed. The key words used were diabetes and bladder dysfunction or cystopathy. Our data and perspective are provided for consideration of the future direction of research.
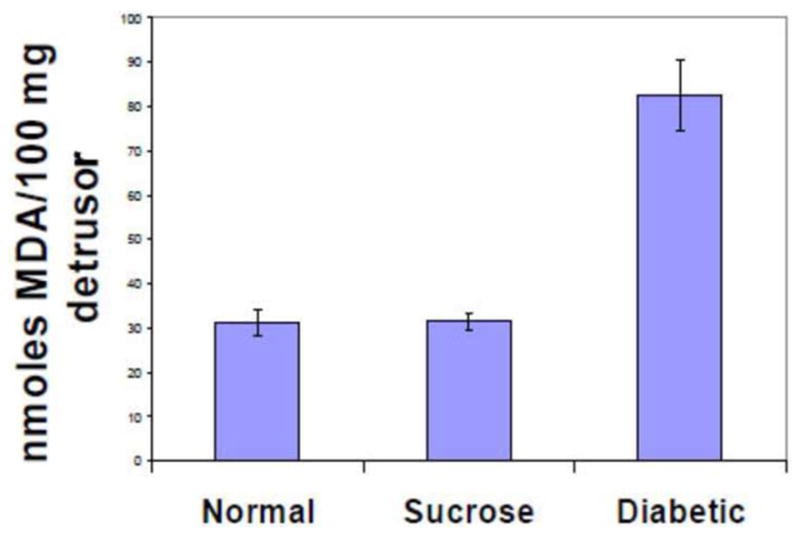
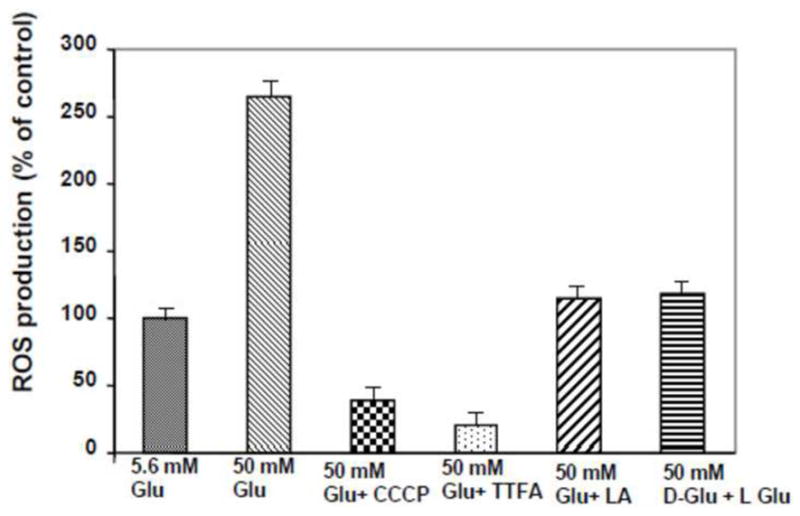
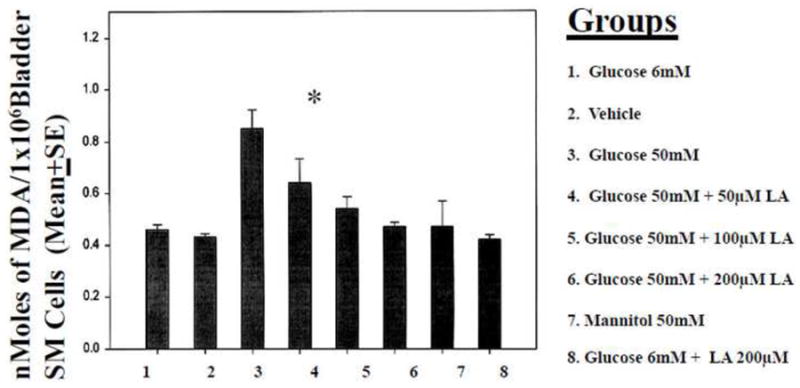
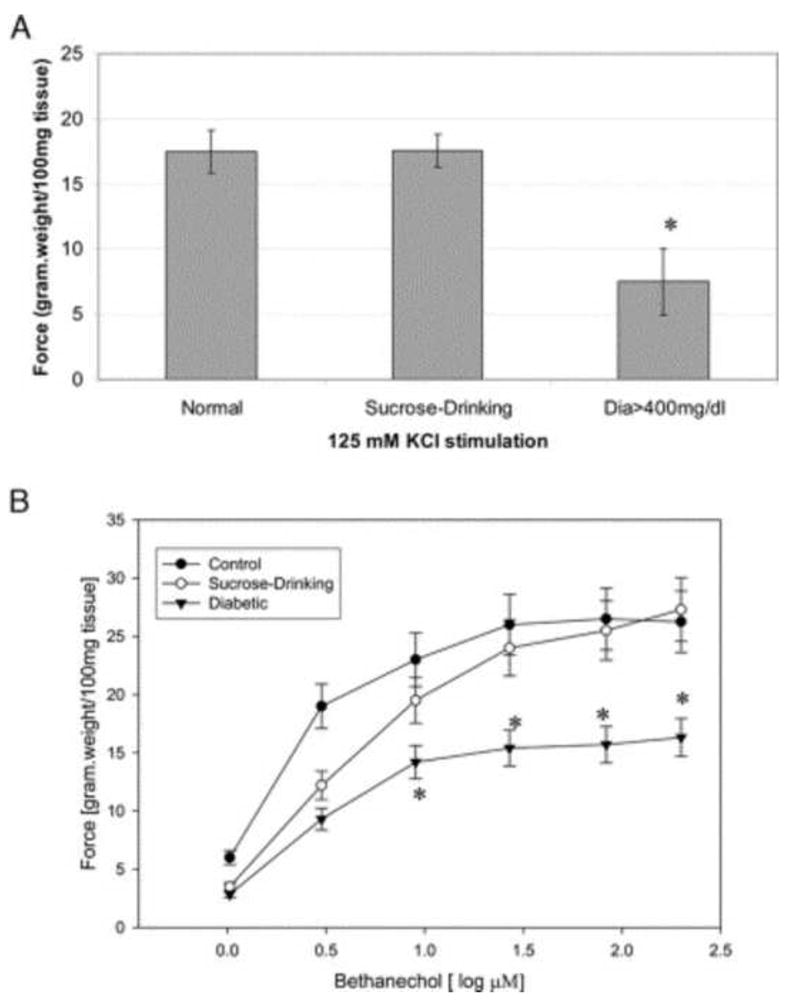
Results: Despite traditional recognition of diabetic bladder dysfunction as a voiding problem characterized by poor emptying and overflow incontinence, recent clinical and experimental evidence indicate storage problems such as urgency and urge incontinence in diabetes mellitus cases. Recent experimental evidence from studies of diabetic bladder dysfunction in small animal models of diabetes mellitus show a temporal effect on diabetic bladder dysfunction. Early phase diabetes mellitus causes compensated bladder function and the late phase causes decompensated bladder function. The temporal theory could plausibly provide the scientific road map to correlate clinical and experimental findings, and identify the role of mechanisms such as polyuria, hyperglycemia, oxidative stress, autonomic neuropathy and decompensation of the bladder contractile apparatus in the creation of clinical and experimental manifestations of diabetic bladder dysfunction.
Conclusions: Diabetic bladder dysfunction includes time dependent manifestations of storage and emptying problems. Identifying mechanistic pathways would lead to the identification of therapeutic intervention.
Figures
References
-
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States. 2005
-
- Bladder Research Progress Review Group. Urologic complications of diabetes mellitus in overcoming bladder disease: a strategic plan for research. A report of the NIH-NIDDK bladder research progress review group. 2004
-
- Bladder Research Progress Review Group. Urologic complications of diabetes mellitus. 2002;133
-
- Daneshgari F, Moore C. Diabetic uropathy. Semin Nephrol. 2006;26:182. - PubMed
-
- Zderic SA, Chacko S, Disanto ME, Wein AJ. Voiding function: relevant anatomy, physiology, pharmacology, and molecular aspects. 2002
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
