

Clinical features of spinal and bulbar muscular atrophy
- PMID: 19846582
- PMCID: PMC2792370
- DOI: 10.1093/brain/awp258
Clinical features of spinal and bulbar muscular atrophy
Abstract
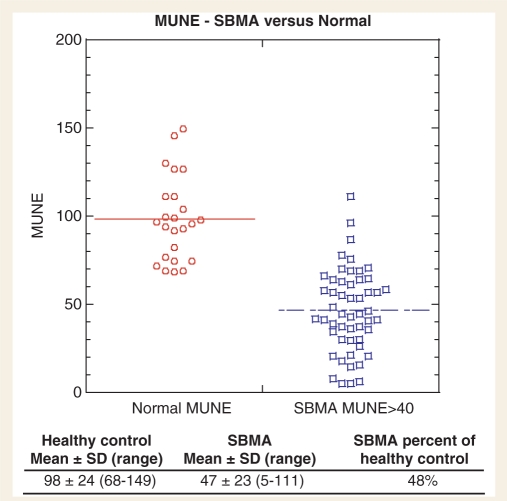
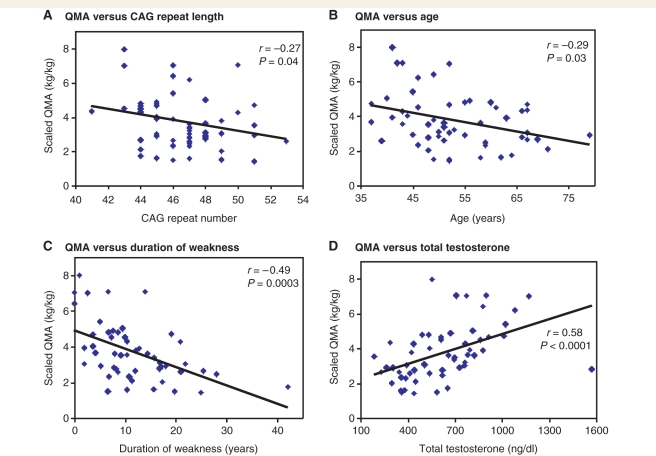
Spinal and bulbar muscular atrophy is an X-linked motor neuron disease caused by a CAG repeat expansion in the androgen receptor gene. To characterize the natural history and define outcome measures for clinical trials, we assessed the clinical history, laboratory findings and muscle strength and function in 57 patients with genetically confirmed disease. We also administered self-assessment questionnaires for activities of daily living, quality of life and erectile function. We found an average delay of over 5 years from onset of weakness to diagnosis. Muscle strength and function correlated directly with serum testosterone levels and inversely with CAG repeat length, age and duration of weakness. Motor unit number estimation was decreased by about half compared to healthy controls. Sensory nerve action potentials were reduced in nearly all subjects. Quantitative muscle assessment and timed 2 min walk may be useful as meaningful indicators of disease status. The direct correlation of testosterone levels with muscle strength indicates that androgens may have a positive effect on muscle function in spinal and bulbar muscular atrophy patients, in addition to the toxic effects described in animal models.
Figures
References
-
- Andres PL, Skerry LM, Thornell B, Portney LG, Finison LJ, Munsat TL. A comparison of three measures of disease progression in ALS. J Neurol Sci. 1996;139 Suppl:64–70. - PubMed
-
- Antonini G, Gragnani F, Romaniello A, Pennisi EM, Morino S, Ceschin V, et al. Sensory involvement in spinal-bulbar muscular atrophy (Kennedy's disease) Muscle Nerve. 2000;23:252–8. - PubMed
-
- Atsuta N, Watanabe H, Ito M, Banno H, Suzuki K, Katsuno M, et al. Natural history of spinal and bulbar muscular atrophy (SBMA): a study of 223 Japanese patients. Brain. 2006;129:1446–55. - PubMed
-
- Banno H, Katsuno M, Suzuki K, Takeuchi Y, Kawashima M, Suga N, et al. Phase 2 trial of leuprorelin in patients with spinal and bulbar muscular atrophy. Ann Neurol. 2009;65:140–50. - PubMed
-
- Brooks D, Davis AM, Naglie G. The feasibility of six-minute and two-minute walk tests in in-patient geriatric rehabilitation. Can J Aging. 2007;26:159–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
