

Clinical diagnosis for discogenic low back pain
- PMID: 19847321
- PMCID: PMC2764347
- DOI: 10.7150/ijbs.5.647
Clinical diagnosis for discogenic low back pain
Erratum in
- Int J Biol Sci. 2010;6(6):613
Abstract
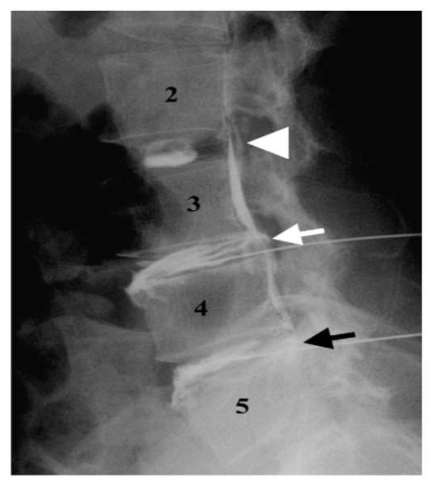
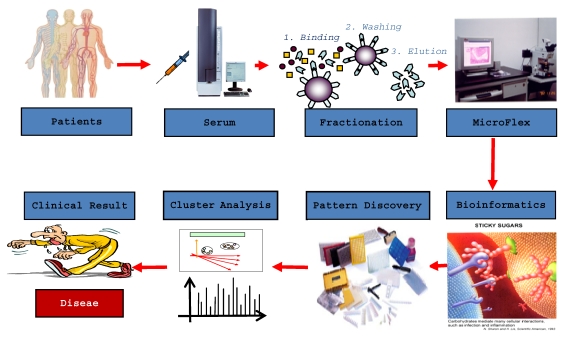
Discogenic lower back pain (DLBP) is the most common type of chronic lower back pain (LBP), accounting for 39% of cases, compared to 30% of cases due to disc herniation, and even lower prevalence rates for other causes, such as zygapophysial joint pain. Only a small proportion (approximately 20%) of LBP cases can be attributed with reasonable certainty to a pathologic or anatomical entity. Thus, diagnosing the cause of LBP represents the biggest challenge for doctors in this field. In this review, we summarize the process of obtaining a clinical diagnosis of DLBP and discuss the potential for serum-based diagnosis in the near future. The use of serum biomarkers to diagnose DLBP is likely to increase the ease of diagnosis as well as produce more accurate and reproducible results.
Keywords: clinical diagnosis; discogenic lower back pain; serum proteomics.
Conflict of interest statement
Conflict of Interest: The authors have declared that no conflict of interest exists.
Figures
References
-
- Sun ZM, Miao L, Zhang YG, Ming L. Association between the -1562 C/T polymorphism of matrix metal proteinase-9 gene and lumbar disc disease in the young adult population in North China. Connect Tissue Res. 2009;50:181–185. - PubMed
-
- Anderson D, Tannoury C. Molecular pathogenic factors in symptomatic disc degeneration. Spine J. 2005;5:260S–266S. - PubMed
-
- Burke JG, Watson RW, McCormack D, Dowling FE, Walsh MG, Fitzpatrick JM. Intervertebral discs which cause low back pain secrete high levels of proinflammatory mediators. J Bone Joint Surg Br. 2002;84:196–201. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
