

Local excision after preoperative chemoradiation results in an equivalent outcome to total mesorectal excision in selected patients with T3 rectal cancer
- PMID: 19847569
- PMCID: PMC3076509
- DOI: 10.1245/s10434-009-0735-7
Local excision after preoperative chemoradiation results in an equivalent outcome to total mesorectal excision in selected patients with T3 rectal cancer
Abstract
Background: We previously reported 26 patients who underwent preoperative chemoradiotherapy (CXRT) for T3 rectal cancer and were subsequently offered full-thickness local excision (LE) as an alternative to total mesorectal excision (TME). At nearly 4 years' follow-up, no difference in outcome was observed. This study compares outcomes in a larger cohort of patients and reevaluates the original 26 patients after longer follow-up.
Methods: Retrospective review was performed of patients who underwent preoperative CXRT (radiation doses of 45, 50.4, or 52.5 Gy with concurrent 5-fluorouracil-based chemotherapy) followed by surgery for T3 rectal cancer. Forty-seven patients underwent LE (Kraske [n = 6] or transanal excision [n = 41]). 473 patients underwent TME (abdominoperineal resection [n = 141] or low anterior resection [n = 332]). Local recurrence, disease-free survival (DFS), disease-specific survival, and overall survival (OS) rates were compared.
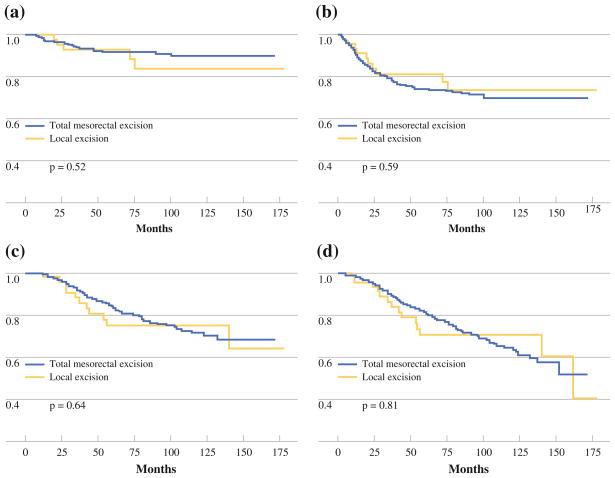
Results: Median follow-up was 63 months for the LE group and 59 months for the TME group. Twenty-three LE patients (49%) had a complete response to CXRT, 17 (36%) had microscopic residual disease, and 7 (15%) had gross residual disease, compared with 108 (23%), 89 (19%), and 276 (58%) TME patients, respectively. There was no significant difference between the 10-year actuarial local recurrence rate for the LE group versus the TME group (10.6% and 7.6%, respectively; P = .52), and no significant difference in DFS, disease-specific survival, or OS rates between groups.
Conclusions: In selected patients who demonstrate an excellent response to preoperative CXRT for T3 rectal cancer, full-thickness LE offers comparable local control, DFS, and OS to that achieved with proctectomy and TME.
Figures
References
-
- Thomas PR, Lindblad AS. Adjuvant postoperative radiotherapy and chemotherapy in rectal carcinoma: a review of the Gastrointestinal Tumor Study Group experience. Radiother Oncol. 1988;13(4):245–52. - PubMed
-
- Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med. 1991;324(11):709–15. - PubMed
-
- Tveit KM, Guldvog I, Hagen S, et al. Randomized controlled trial of postoperative radiotherapy and short-term time-scheduled 5-fluorouracil against surgery alone in the treatment of Dukes B and C rectal cancer. Norwegian Adjuvant Rectal Cancer Project Group. Br J Surg. 1997;84(8):1130–5. - PubMed
-
- Bosset JF, Collette L, Calais G, et al. Chemotherapy with pre-operative radiotherapy in rectal cancer. N Engl J Med. 2006;355(11):1114–23. - PubMed
-
- Gerard JP, Conroy T, Bonnetain F, et al. Preoperative radio-therapy with or without concurrent fluorouracil and leucovorin in T3–4 rectal cancers: results of FFCD 9203. J Clin Oncol. 2006;24(28):4620–5. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
