

Identification of a pseudo-outbreak of Clostridium difficile infection (CDI) and the effect of repeated testing, sensitivity, and specificity on perceived prevalence of CDI
- PMID: 19848606
- PMCID: PMC3598603
- DOI: 10.1086/648089
Identification of a pseudo-outbreak of Clostridium difficile infection (CDI) and the effect of repeated testing, sensitivity, and specificity on perceived prevalence of CDI
Abstract
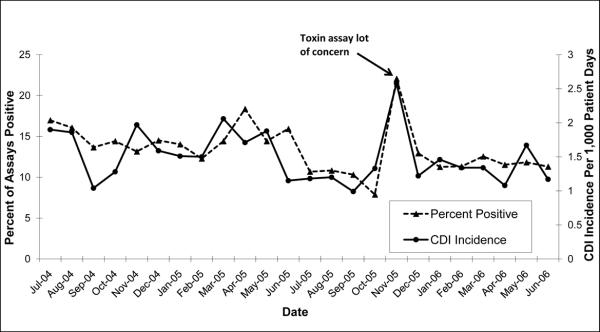
Objective: To describe a pseudo-outbreak of Clostridium difficile infection (CDI) caused by a faulty toxin assay lot and to determine the effect of sensitivity, specificity, and repeated testing for C. difficile on perceived CDI burden, positive predictive value, and false-positive results.
Design: Outbreak investigation and criterion standard.
Patients: Patients hospitalized at a tertiary care hospital who had at least 1 toxin assay for detection of C. difficile performed during the period from July 1, 2004, through June 30, 2006.
Methods: The run control chart method and the chi(2) test were used to compare CDI rates and the proportion of positive test results before, during, and after the pseudo-outbreak. The effect of repeated testing was evaluated by using 3 hypothetical models with a sample of 10,000 patients and various assay sensitivity and specificity estimates.
Results: In November of 2005, the CDI rate at the hospital increased from 1.5 to 2.6 cases per 1,000 patient-days (P < .01), and the proportion of positive test results increased from 13.6% to 22.1% (P < .01). An investigation revealed a pseudo-outbreak caused by a faulty toxin assay lot. A decrease of only 1.2% in the specificity of the toxin assay would result in a 32% increase in perceived incidence of CDI at this institution. When calculated by use of the manufacturer's stated specificity and sensitivity and this institution's testing practices, the positive predictive value of the test decreased from 80.6% to 4.1% for patients who received 3 tests.
Conclusion: Specificity is as important as sensitivity when testing for CDI. False-positive CDI cases can drain hospital resources and adversely affect patients. Repeated testing for C. difficile should be performed with caution.
Figures
References
-
- Goorhuis A, Van der KT, Vaessen N, Dekker FW, Van den BR, Harmanus C, et al. Spread and epidemiology of Clostridium difficile polymerase chain reaction ribotype 027/toxinotype III in The Netherlands. Clin Infect Dis. 2007;45(6):695–703. - PubMed
-
- Loo VG, Poirier L, Miller MA, Oughton M, Libman MD, Michaud S, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005;353(23):2442–2449. - PubMed
-
- Gerding DN. New definitions will help, but cultures are critical for resolving unanswered questions about Clostridium difficile. Infect Control Hosp Epidemiol. 2007;28(2):113–115. - PubMed
-
- Peterson LR, Manson RU, Paule SM, Hacek DM, Robicsek A, Thomson RB, Jr., et al. Detection of toxigenic Clostridium difficile in stool samples by real-time polymerase chain reaction for the diagnosis of C. difficile-associated diarrhea. Clin Infect Dis. 2007;45(9):1152–1160. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
