

Concomitant medication use can confound interpretation of the combined dexamethasone-corticotropin releasing hormone test in Cushing's syndrome
- PMID: 19850679
- PMCID: PMC2795659
- DOI: 10.1210/jc.2009-1500
Concomitant medication use can confound interpretation of the combined dexamethasone-corticotropin releasing hormone test in Cushing's syndrome
Abstract
Context: The ability of combined dexamethasone-corticotropin releasing hormone (Dex-CRH) testing to distinguish pseudo-Cushing's syndrome (PCS) from Cushing's syndrome is controversial. One factor potentially impairing diagnostic efficacy is the concomitant use of commonly prescribed medications that may alter dexamethasone metabolism.
Objective: Our objective was to assess the diagnostic accuracy of the Dex-CRH test and evaluate the potential impact of concomitant drugs.
Design: The study was a retrospective one.
Participants: Participants included 101 patients [60 Cushing's disease (CD); 41 PCS] who underwent 112 Dex-CRH tests. Patients were divided into two groups, depending on use of medications potentially interfering with dexamethasone metabolism: 58 tests were classified as No Meds (32 CD; 26 PCS) and 54 as Meds (34 CD; 20 PCS). The latter group was further subdivided into patients taking one medication vs. those taking multiple medications.
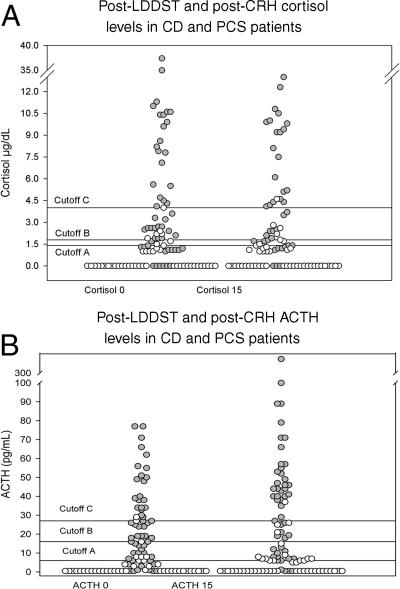
Main outcome measures: Diagnostic accuracy of different serum cortisol and ACTH thresholds at baseline and 15 min after CRH injection was assessed.
Results: The specificity of a baseline post-low-dose-dexamethasone-suppressed test cortisol lower than 1.4 microg/dl (38 nmol/liter) was significantly higher in the No Meds vs. the Meds group (P = 0.014). Sensitivity and specificity using a post-CRH cortisol cutoff of 1.4 microg/dl (38 nmol/liter) were 93.1% (95% confidence interval = 88.4-97.8) and 92.3% (95% confidence interval = 87-97.6) in the No Meds group. The specificity of a cortisol lower than 1.4 microg/dl (38 nmol/l) at 15 min after CRH was significantly higher in patients taking only one medication vs. those on multidrug treatment (P < 0.05).
Conclusions: Medications commonly prescribed in hypercortisolemic patients undergoing Dex-CRH testing may contribute to the variable diagnostic accuracy of this test. Prospective studies to address this issue are needed.
Figures
Similar articles
-
Corticotropin-releasing hormone stimulation following low-dose dexamethasone administration. A new test to distinguish Cushing's syndrome from pseudo-Cushing's states.JAMA. 1993 May 5;269(17):2232-8. JAMA. 1993. PMID: 8386285
-
The dexamethasone-suppressed corticotropin-releasing hormone stimulation test and the desmopressin test to distinguish Cushing's syndrome from pseudo-Cushing's states.Clin Endocrinol (Oxf). 2007 Feb;66(2):251-7. doi: 10.1111/j.1365-2265.2006.02717.x. Clin Endocrinol (Oxf). 2007. PMID: 17223996 Clinical Trial.
-
Reevaluation of the combined dexamethasone suppression-corticotropin-releasing hormone test for differentiation of mild cushing's disease from pseudo-Cushing's syndrome.J Clin Endocrinol Metab. 2007 Nov;92(11):4290-3. doi: 10.1210/jc.2006-2829. Epub 2007 Jul 17. J Clin Endocrinol Metab. 2007. PMID: 17635947
-
The conundrum of differentiating Cushing's syndrome from non-neoplastic hypercortisolism: a systematic review and meta-analysis.Pituitary. 2024 Aug;27(4):345-359. doi: 10.1007/s11102-024-01408-w. Epub 2024 Jun 18. Pituitary. 2024. PMID: 38888685
-
Differential diagnosis and management of Cushing's syndrome.Annu Rev Med. 1996;47:443-61. doi: 10.1146/annurev.med.47.1.443. Annu Rev Med. 1996. PMID: 8712794 Review.
Cited by
-
Markers of Subclinical Cardiovascular Disease in Patients with Adrenal Incidentaloma.Medicina (Kaunas). 2020 Feb 10;56(2):69. doi: 10.3390/medicina56020069. Medicina (Kaunas). 2020. PMID: 32050625 Free PMC article. Review.
-
Are comorbidities of patients with adrenal incidentaloma tied to sex?Front Endocrinol (Lausanne). 2024 May 14;15:1385808. doi: 10.3389/fendo.2024.1385808. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38808113 Free PMC article.
-
Molecular Derangements and the Diagnosis of ACTH-Dependent Cushing's Syndrome.Endocr Rev. 2022 Sep 26;43(5):852-877. doi: 10.1210/endrev/bnab046. Endocr Rev. 2022. PMID: 34849663 Free PMC article. Review.
-
Secondary Arterial Hypertension: From Routine Clinical Practice to Evidence in Patients with Adrenal Tumor.High Blood Press Cardiovasc Prev. 2018 Dec;25(4):345-354. doi: 10.1007/s40292-018-0288-6. Epub 2018 Nov 10. High Blood Press Cardiovasc Prev. 2018. PMID: 30415425 Review.
-
Role of Cytochrome P450 2C9 in COVID-19 Treatment: Current Status and Future Directions.Eur J Drug Metab Pharmacokinet. 2023 May;48(3):221-240. doi: 10.1007/s13318-023-00826-8. Epub 2023 Apr 24. Eur J Drug Metab Pharmacokinet. 2023. PMID: 37093458 Free PMC article. Review.
References
-
- Findling JW, Raff H 2006 Cushing’s syndrome: important issues in diagnosis and management. J Clin Endocrinol Metab 91:3746–3753 - PubMed
-
- Catargi B, Rigalleau V, Poussin A, Ronci-Chaix N, Bex V, Vergnot V, Gin H, Roger P, Tabarin A 2003 Occult Cushing’s syndrome in type 2 diabetes. J Clin Endocrinol Metab 88:5808–5813 - PubMed
-
- Chiodini I, Mascia ML, Muscarella S, Battista C, Minisola S, Arosio M, Santini SA, Guglielmi G, Carnevale V, Scillitani A 2007 Subclinical hypercortisolism among outpatients referred for osteoporosis. Ann Intern Med 147: 541–548 - PubMed
-
- Yanovski JA, Cutler Jr GB, Chrousos GP, Nieman LK 1993 Corticotropin-releasing hormone stimulation following low-dose dexamethasone administration. A new test to distinguish Cushing’s syndrome from pseudo-Cushing’s states. JAMA 269: 2232–2238 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
