

Protected endovascular revascularization of subacute and chronic total occlusion of the internal carotid artery
- PMID: 19850764
- PMCID: PMC7963968
- DOI: 10.3174/ajnr.A1843
Protected endovascular revascularization of subacute and chronic total occlusion of the internal carotid artery
Abstract
Background and purpose: The natural course of symptomatic carotid artery occlusion with hemodynamic impairment is poor. Surgical revascularization may improve the outcome; however, its efficacy has not been established yet. The goal of this study was to characterize the technical and clinical outcomes following endovascular recanalization of the ICA under cerebral circulatory protection.
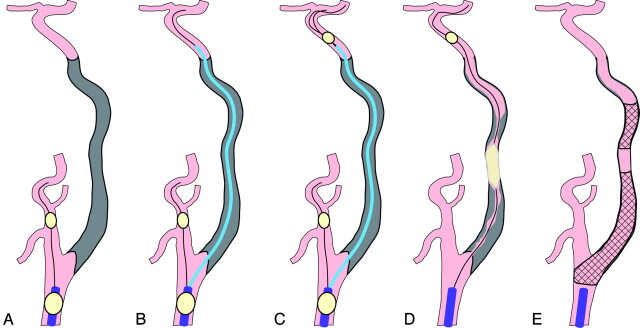
Materials and methods: Endovascular recanalization was attempted in 8 patients with symptomatic ICA occlusions. The duration of the occlusion ranged from 7 days to 7 months (mean, 2.5 months), and the mean length of the occlusion was 95 mm. Cerebral hemodynamics ipsilateral to the side of the occlusion were severely impaired in all patients. The endovascular procedure was performed under total cerebral circulatory protection, beginning with proximal protection with a subsequent switch to distal protection after successful guidewire passage.
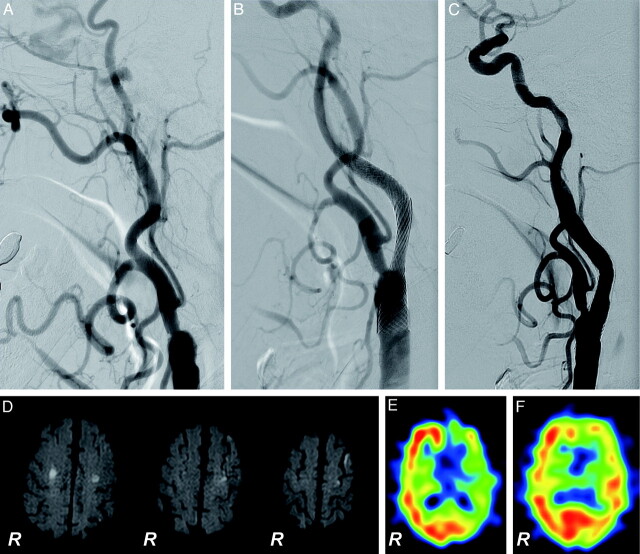
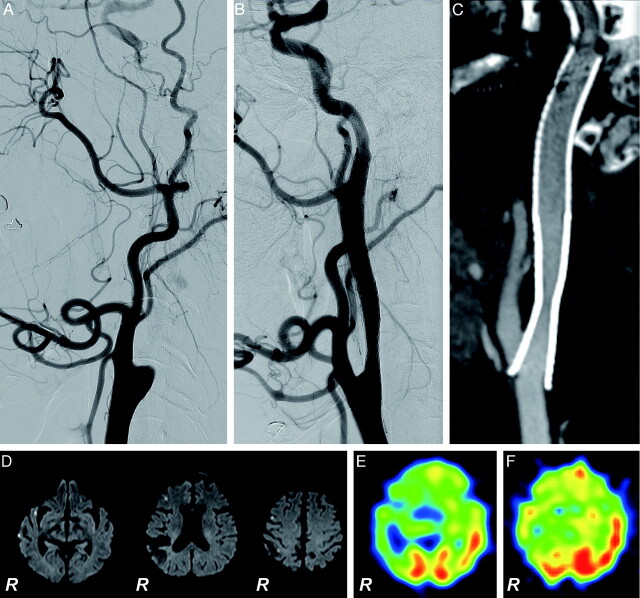
Results: The occlusion was recanalized successfully in 7 of 8 patients (88%), resulting in improvement of ipsilateral cerebral hemodynamics without symptomatic stroke. Small asymptomatic ischemic lesions were detected in 6 of 8 patients (75%) on DWI, and 1 patient developed a mild groin hematoma. Ischemic episodes did not recur during the mean follow-up period of 19 months. However, 1 patient experienced asymptomatic reocclusion, which was re-treated successfully without complications, while another patient developed mild retinal hemorrhage at 3 months after the procedure due to the combination of antiplatelet and anticoagulant therapy.
Conclusions: Endovascular revascularization of an ICA occlusion is feasible and well-tolerated in patients with subacute or chronic total occlusion of the ICA.
Figures
Similar articles
-
Endovascular recanalization for symptomatic subacute and chronic intracranial large artery occlusion of the anterior circulation: initial experience and technical considerations.Neuroradiology. 2019 Jul;61(7):833-842. doi: 10.1007/s00234-019-02205-0. Epub 2019 May 1. Neuroradiology. 2019. PMID: 31044262
-
Staged endovascular recanalization for symptomatic atherosclerotic non-acutely occluded internal carotid artery.Interv Neuroradiol. 2025 Apr;31(2):208-219. doi: 10.1177/15910199231162666. Epub 2023 Mar 7. Interv Neuroradiol. 2025. PMID: 36883208 Free PMC article.
-
Feasibility of endovascular recanalization for symptomatic cervical internal carotid artery occlusion.J Am Coll Cardiol. 2007 Feb 20;49(7):765-71. doi: 10.1016/j.jacc.2006.11.029. Epub 2007 Feb 5. J Am Coll Cardiol. 2007. PMID: 17306705 Clinical Trial.
-
Revascularization of tandem occlusions in acute ischemic stroke: review of the literature and illustrative case.Neurosurg Focus. 2017 Apr;42(4):E15. doi: 10.3171/2017.1.FOCUS16521. Neurosurg Focus. 2017. PMID: 28366063 Review.
-
Overview of evidence on emergency carotid stenting in patients with acute ischemic stroke due to tandem occlusions: a systematic review and meta-analysis.J Cardiovasc Surg (Torino). 2019 Dec;60(6):693-702. doi: 10.23736/S0021-9509.18.10312-0. Epub 2018 Jan 23. J Cardiovasc Surg (Torino). 2019. PMID: 29363895
Cited by
-
Hybrid operation to revascularize long-segment occluded internal carotid artery prevent further ischemic events.Neuroradiology. 2019 Feb;61(2):217-224. doi: 10.1007/s00234-018-2145-7. Epub 2018 Dec 14. Neuroradiology. 2019. PMID: 30552444
-
Management of De Novo Carotid Stenosis and Postintervention Restenosis-Carotid Endarterectomy Versus Carotid Artery Stenting-a Review of Literature.Transl Stroke Res. 2019 Oct;10(5):460-474. doi: 10.1007/s12975-019-00693-z. Epub 2019 Feb 22. Transl Stroke Res. 2019. PMID: 30793257 Review.
-
Association between proximal internal carotid artery steno-occlusive disease and diffuse wall thickening in its petrous segment: a magnetic resonance vessel wall imaging study.Neuroradiology. 2017 May;59(5):485-490. doi: 10.1007/s00234-017-1825-z. Epub 2017 Mar 29. Neuroradiology. 2017. PMID: 28357461
-
Stroke: Evolution of newer treatment modalities for acute ischemic stroke.World J Clin Cases. 2024 Oct 6;12(28):6137-6147. doi: 10.12998/wjcc.v12.i28.6137. World J Clin Cases. 2024. PMID: 39371560 Free PMC article.
-
Recanalization of chronic long-segment occlusion of the internal carotid artery with endovascular and hybrid surgery.Sci Rep. 2023 Oct 9;13(1):17026. doi: 10.1038/s41598-023-44406-x. Sci Rep. 2023. PMID: 37813974 Free PMC article.
References
-
- Klijn CJ, Kappelle LJ, Tulleken CA, et al. . Symptomatic carotid artery occlusion: a reappraisal of hemodynamic factors. Stroke 1997;28:2084–93 - PubMed
-
- Grubb RL, Jr, Derdeyn CP, Fritsch SM, et al. . Importance of hemodynamic factors in the prognosis of symptomatic carotid occlusion. JAMA 1998;280:1055–60 - PubMed
-
- Kuroda S, Houkin K, Kamiyama H, et al. . Long-term prognosis of medically treated patients with internal carotid or middle cerebral artery occlusion: can acetazolamide test predict it? Stroke 2001;32:2110–16 - PubMed
-
- Hafner CD, Tew JM. Surgical management of the totally occluded internal carotid artery: a ten-year study. Surgery 1981;89:710–17 - PubMed
-
- Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke: results of an international randomized trial—the EC/IC Bypass Study Group. N Engl J Med 1985;313:1191–200 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous