

Safety and efficacy of oral DMSA therapy for children with autism spectrum disorders: Part A--medical results
- PMID: 19852789
- PMCID: PMC2774660
- DOI: 10.1186/1472-6904-9-16
Safety and efficacy of oral DMSA therapy for children with autism spectrum disorders: Part A--medical results
Abstract
Background: This study investigated the effect of oral dimercapto succinic acid (DMSA) therapy for children with autism spectrum disorders ages 3-8 years.
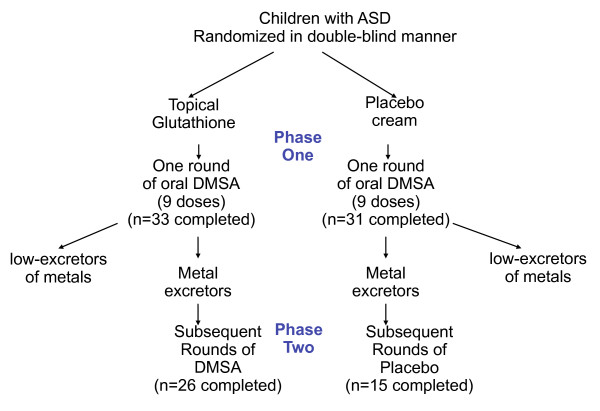
Methods: Phase 1 involved 65 children who received one round of DMSA (3 days). Participants who had high urinary excretion of toxic metals were selected to continue on to phase 2. In phase 2, 49 participants were randomly assigned in a double-blind design to receive an additional 6 rounds of either DMSA or placebo.
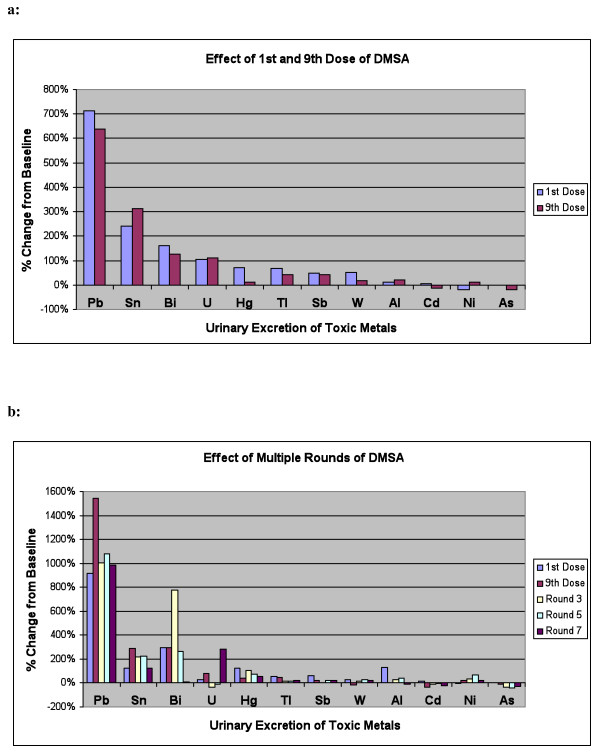
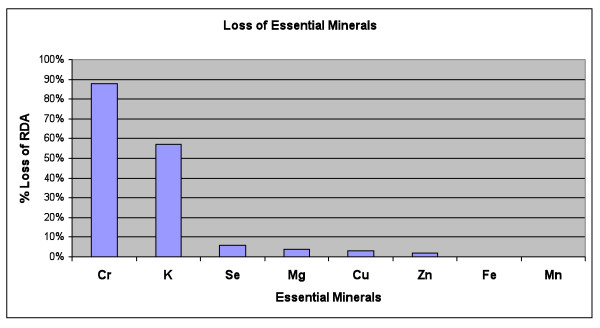
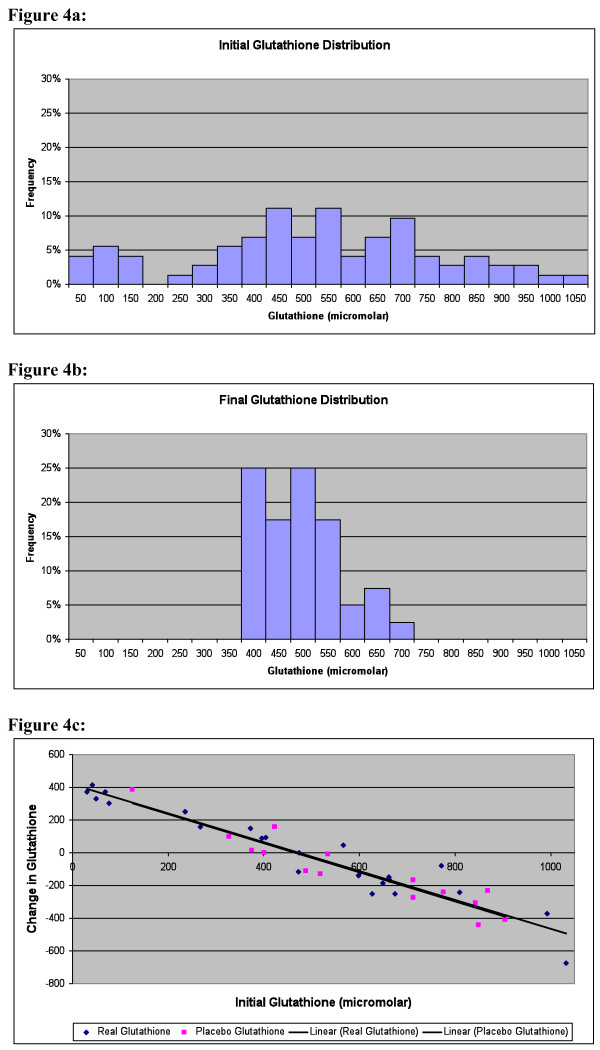
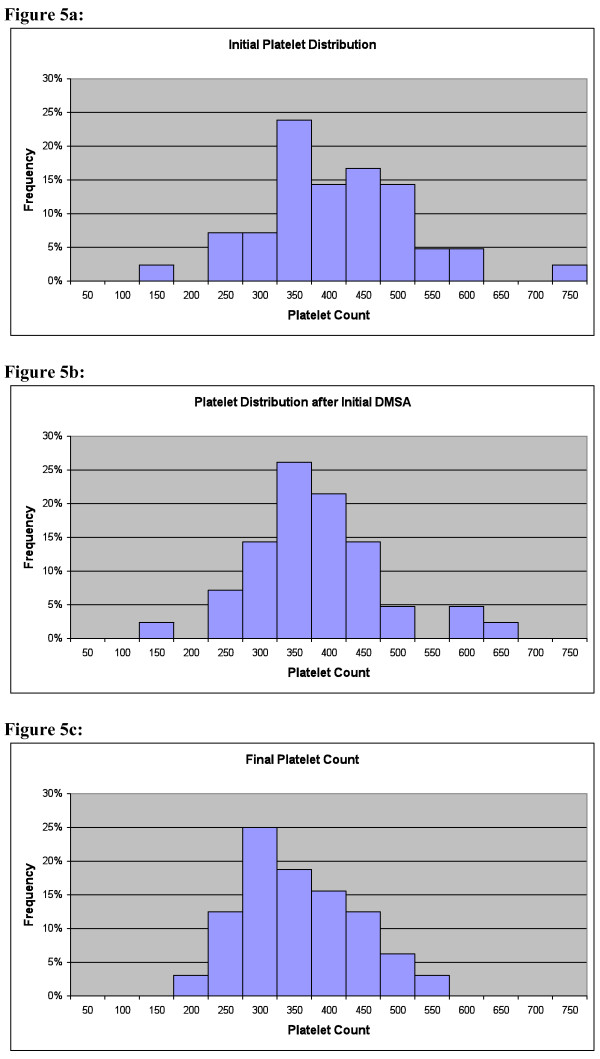
Results: DMSA greatly increased the excretion of lead, substantially increased excretion of tin and bismuth, and somewhat increased the excretion of thallium, mercury, antimony, and tungsten. There was some increase in urinary excretion of essential minerals, especially potassium and chromium. The Phase 1 single round of DMSA led to a dramatic normalization of RBC glutathione in almost all cases, and greatly improved abnormal platelet counts, suggesting a significant decrease in inflammation.
Conclusion: Overall, DMSA therapy seems to be reasonably safe, effective in removing several toxic metals (especially lead), dramatically effective in normalizing RBC glutathione, and effective in normalizing platelet counts. Only 1 round (3 days) was sufficient to improve glutathione and platelets. Additional rounds increased excretion of toxic metals.
Figures
References
-
- Rowland IR, Robinson RD, Doherty RA. Effect of diet on mercury metabolism and excretion in mice given methylmercury: role of gut flora. Arch Env Health. 1984;39:401–408. - PubMed
-
- James SJ, Cutler P, Melnyk S, Jernigan S, Janak L, Gaylor DW, Neubrander JA. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am J Clin Nutr. 2004;80:1611–7. - PubMed
-
- James SJ, Melnyk S, Jernigan S, Cleves MA, Halsted CH, Wong DH, Cutler P, Bock K, Boris M, Bradstreet JJ, Baker SM, Gaylor DW. Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am J Med Genet B Neuropsychiatr Genet. 2006;141:947–956. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
