

Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial
- PMID: 19853510
- PMCID: PMC3042271
- DOI: 10.1016/S1470-2045(09)70284-0
Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial
Erratum in
- Lancet Oncol. 2010 Jan;11(1):14
Abstract
Background: High-dose dexamethasone is a mainstay of therapy for multiple myeloma. We studied whether low-dose dexamethasone in combination with lenalidomide is non-inferior to and has lower toxicity than high-dose dexamethasone plus lenalidomide.
Methods: Patients with untreated symptomatic myeloma were randomly assigned in this open-label non-inferiority trial to lenalidomide 25 mg on days 1-21 plus dexamethasone 40 mg on days 1-4, 9-12, and 17-20 of a 28-day cycle (high dose), or lenalidomide given on the same schedule with dexamethasone 40 mg on days 1, 8, 15, and 22 of a 28-day cycle (low dose). After four cycles, patients could discontinue therapy to pursue stem-cell transplantation or continue treatment until disease progression. The primary endpoint was response rate after four cycles assessed with European Group for Blood and Bone Marrow Transplant criteria. The non-inferiority margin was an absolute difference of 15% in response rate. Analysis was by modified intention to treat. This trial is registered with ClinicalTrials.gov, number NCT00098475.
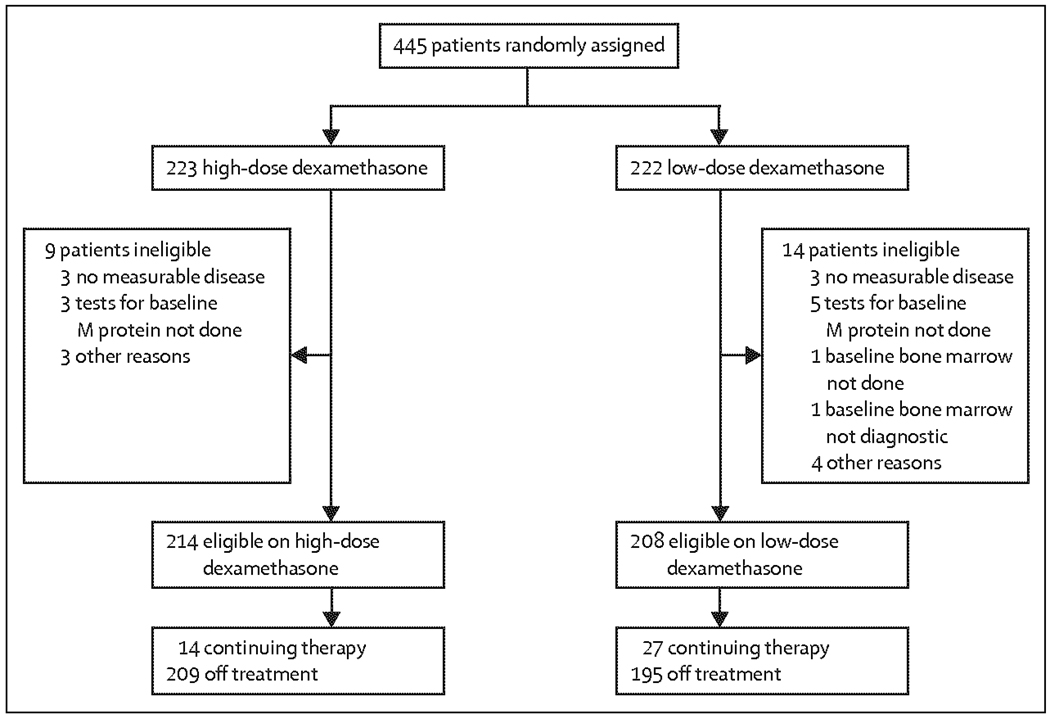
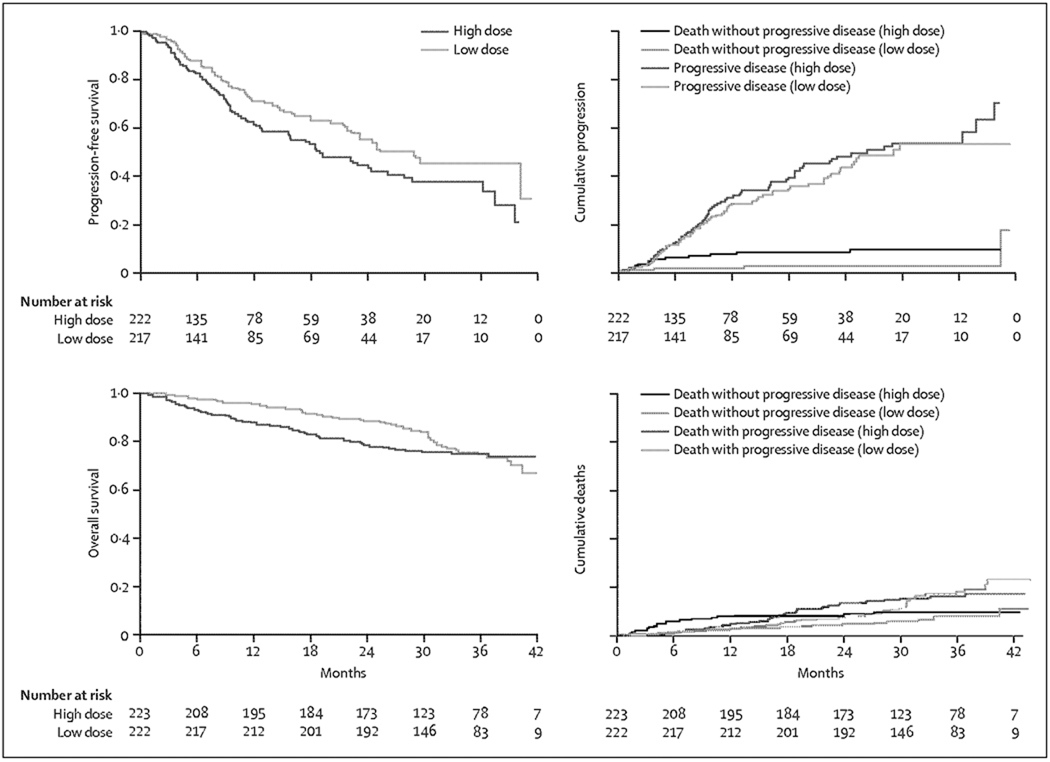
Findings: 445 patients were randomly assigned: 223 to high-dose and 222 to low-dose regimens. 169 (79%) of 214 patients receiving high-dose therapy and 142 (68%) of 205 patients on low-dose therapy had complete or partial response within four cycles (odds ratio 1.75, 80% CI 1.30-2.32; p=0.008). However, at the second interim analysis at 1 year, overall survival was 96% (95% CI 94-99) in the low-dose dexamethasone group compared with 87% (82-92) in the high-dose group (p=0.0002). As a result, the trial was stopped and patients on high-dose therapy were crossed over to low-dose therapy. 117 patients (52%) on the high-dose regimen had grade three or worse toxic effects in the first 4 months, compared with 76 (35%) of the 220 on the low-dose regimen for whom toxicity data were available (p=0.0001), 12 of 222 on high dose and one of 220 on low-dose dexamethasone died in the first 4 months (p=0.003). The three most common grade three or higher toxicities were deep-vein thrombosis, 57 (26%) of 223 versus 27 (12%) of 220 (p=0.0003); infections including pneumonia, 35 (16%) of 223 versus 20 (9%) of 220 (p=0.04), and fatigue 33 (15%) of 223 versus 20 (9%) of 220 (p=0.08), respectively.
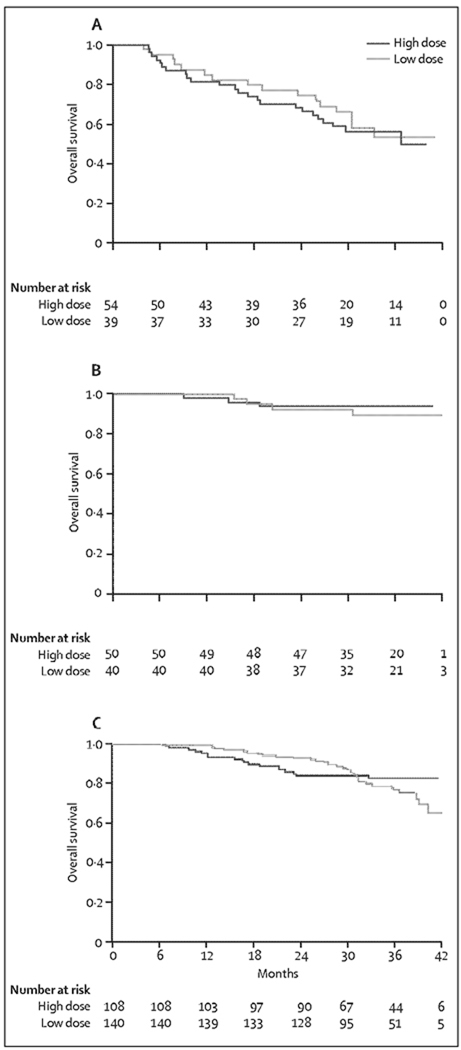
Interpretation: Lenalidomide plus low-dose dexamethasone is associated with better short-term overall survival and with lower toxicity than lenalidomide plus high-dose dexamethasone in patients with newly diagnosed myeloma.
Funding: National Cancer Institute, Rockville, MD, USA.
Copyright (c) 2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DHV has served on the speaker’s bureau for Millennium, Celgene, and Ortho-Biotech and on advisory boards for Celgene and Amgen. MEW has received research support from Celgene. RA has received research support and honoraria from Celgene, Millennium, and Novartis. RF has served as a consultant for Amgen, Halozyme, Otsuka, BMS, and Genzyme, has received research funding from Cylene and Pfizer, and has received honoraria from Celgene and Millennium. NSC has received research support from Millennium. The other authors declared no conflicts of interest.
Figures

Comment in
-
Towards a new standard of care for patients with myeloma?Lancet Oncol. 2010 Jan;11(1):3-4. doi: 10.1016/S1470-2045(09)70313-4. Epub 2009 Oct 21. Lancet Oncol. 2010. PMID: 19853511 No abstract available.
References
-
- Attal M, Harousseau JL, Stoppa AM, et al. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Français du Myćlomc. N Engl J Med. 1996;335:91–97. - PubMed
-
- Child JA, Morgan GJ, Davies FE, et al. High-dose chemotherapy with hematopoictic stem-cell rescue for multiple myeloma. N Engl J Med. 2003;348:1875–1883. - PubMed
-
- Attal M, Harousseau JL, Facon T, et al. Single versus double autologous stem-cell transplantation for multiple myeloma. N Engl J Med. 2003;349:2495–2502. - PubMed
-
- Singhal S, Mehta J, Desikan R, et al. Antirumor activity of thalidomide in refractory multiple myeloma. N Engl J Med. 1999;341:1565–1571. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
