

Drug-specific risk of tuberculosis in patients with rheumatoid arthritis treated with anti-TNF therapy: results from the British Society for Rheumatology Biologics Register (BSRBR)
- PMID: 19854715
- PMCID: PMC2927681
- DOI: 10.1136/ard.2009.118935
Drug-specific risk of tuberculosis in patients with rheumatoid arthritis treated with anti-TNF therapy: results from the British Society for Rheumatology Biologics Register (BSRBR)
Abstract
Background: The risk of tuberculosis (TB) in patients with rheumatoid arthritis (RA) is thought to be increased following anti-tumour necrosis factor (anti-TNF) therapy, with a proposed differential risk between the anti-TNF drugs etanercept (ETA), infliximab (INF) and adalimumab (ADA).
Objective: To compare directly the risk between drugs, to explore time to event, site of infection and the role of ethnicity.
Methods: Data from the British Society for Rheumatology Biologics Register (BSRBR), a national prospective observational study, were used to compare TB rates in 10 712 anti-TNF treated patients (3913 ETA, 3295 INF, 3504 ADA) and 3232 patients with active RA treated with traditional disease-modifying antirheumatic drugs.
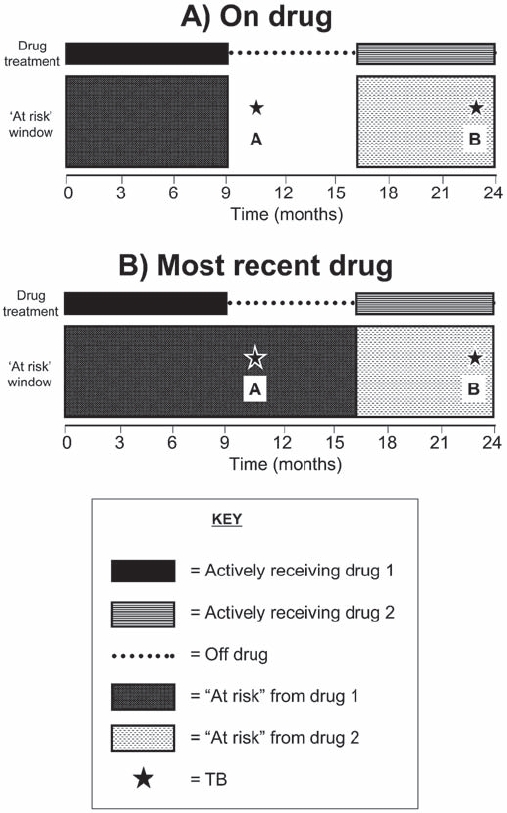
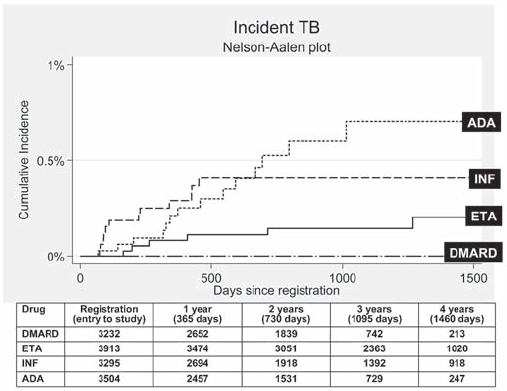
Results: To April 2008, 40 cases of TB were reported, all in the anti-TNF cohort. The rate of TB was higher for the monoclonal antibodies ADA (144 events/100,000 person-years) and INF (136/100,000 person-years) than for ETA (39/100,000 person-years). After adjustment, the incidence rate ratio compared with ETA-treated patients was 3.1 (95% CI 1.0 to 9.5) for INF and 4.2 (1.4 to 12.4) for ADA. The median time to event was lowest for INF (5.5 months) compared with ETA (13.4 months) and ADA (18.5 months). 13/40 cases occurred after stopping treatment. 25/40 (62%) cases were extrapulmonary, of which 11 were disseminated. Patients of non-white ethnicity had a sixfold increased risk of TB compared with white patients treated with anti-TNF therapy.
Conclusion: The rate of TB in patients with RA treated with anti-TNF therapy was three- to fourfold higher in patients receiving INF and ADA than in those receiving ETA.
Conflict of interest statement
Figures
References
-
- Maini R, St Clair EW, Breedveld F, et al. Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. ATTRACT Study Group. Lancet 1999;354:1932–9 - PubMed
-
- Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. [see comment]. N Engl J Med 2001;345:1098–104 - PubMed
-
- Mohan AK, Cote TR, Block JA, et al. Tuberculosis following the use of etanercept, a tumor necrosis factor inhibitor. [see comment]. Clin Infect Dis 2004;39:295–9 - PubMed
-
- Wallis RS, Broder MS, Wong JY, et al. Granulomatous infectious diseases associated with tumor necrosis factor antagonists. [see comment]. Clin Infect Dis 2004;38:1261–5 - PubMed
-
- Wallis RS, Broder M, Wong J, et al. Granulomatous infections due to tumor necrosis factor blockade: correction. Clin Infect Dis 2004;39:1254–5 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
