

Hypothermia and postconditioning after cardiopulmonary resuscitation reduce cardiac dysfunction by modulating inflammation, apoptosis and remodeling
- PMID: 19855846
- PMCID: PMC2764338
- DOI: 10.1371/journal.pone.0007588
Hypothermia and postconditioning after cardiopulmonary resuscitation reduce cardiac dysfunction by modulating inflammation, apoptosis and remodeling
Abstract
Background: Mild therapeutic hypothermia following cardiac arrest is neuroprotective, but its effect on myocardial dysfunction that is a critical issue following resuscitation is not clear. This study sought to examine whether hypothermia and the combination of hypothermia and pharmacological postconditioning are cardioprotective in a model of cardiopulmonary resuscitation following acute myocardial ischemia.
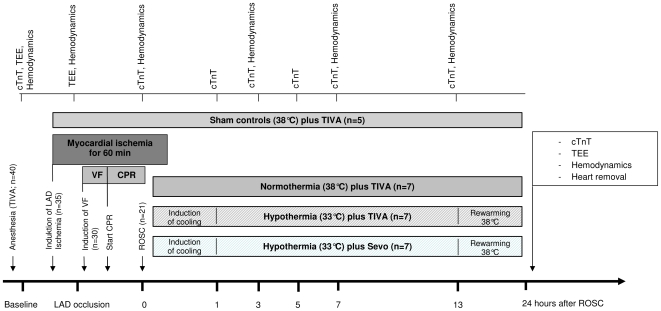
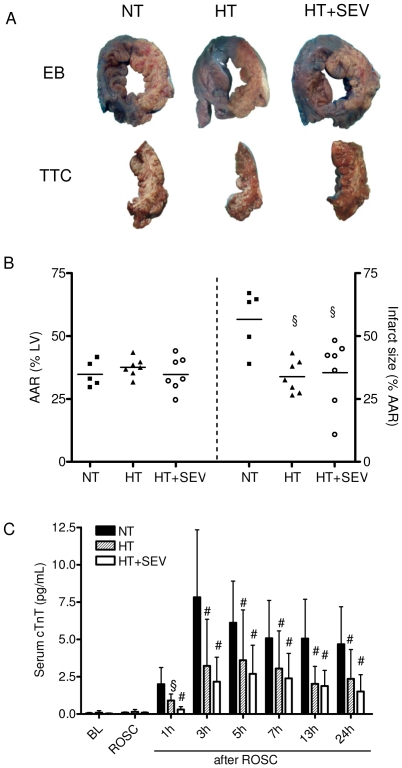
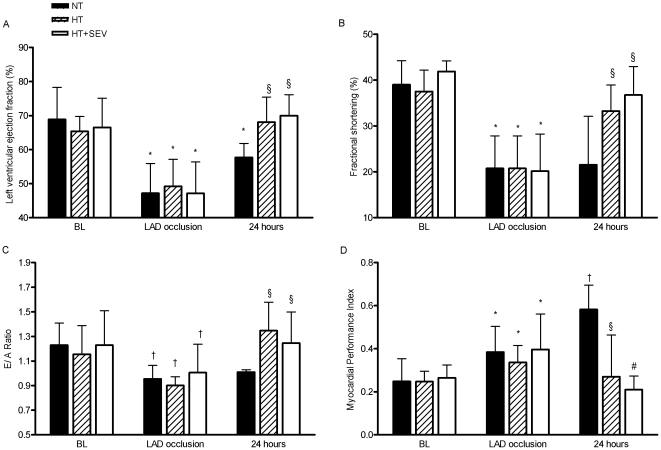
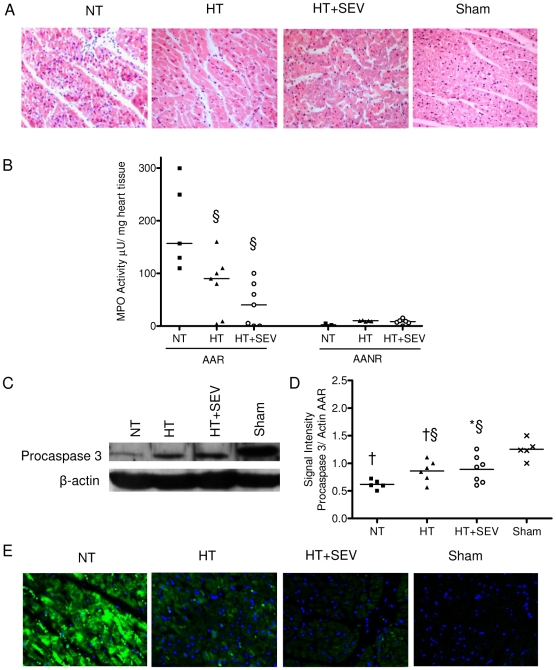
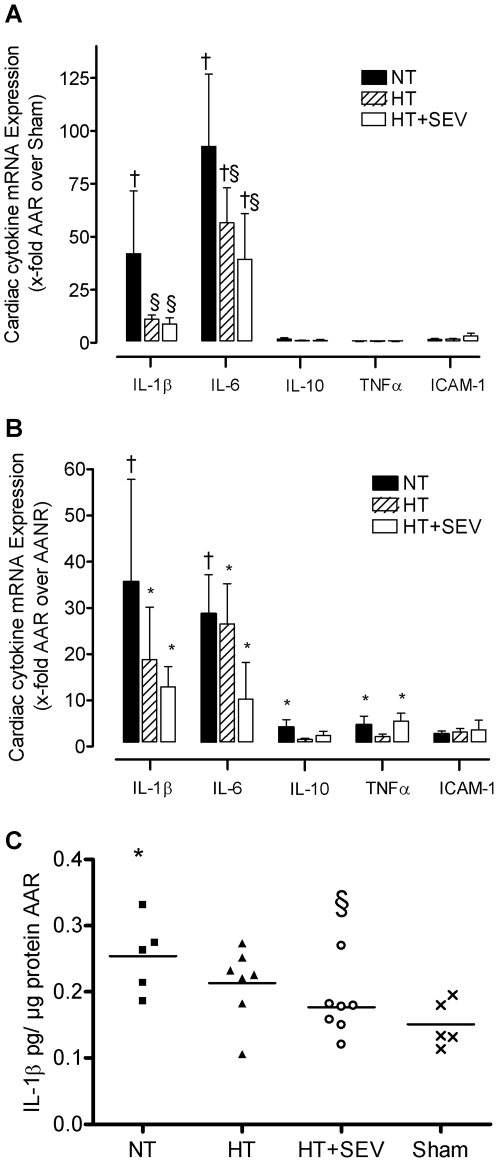
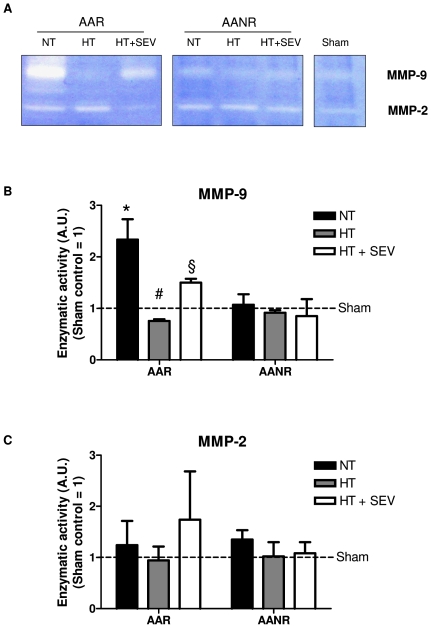
Methodology/principal findings: Thirty pigs (28-34 kg) were subjected to cardiac arrest following left anterior descending coronary artery ischemia. After 7 minutes of ventricular fibrillation and 2 minutes of basic life support, advanced cardiac life support was started according to the current AHA guidelines. After successful return of spontaneous circulation (n = 21), coronary perfusion was reestablished after 60 minutes of occlusion, and animals were randomized to either normothermia at 38 degrees C, hypothermia at 33 degrees C or hypothermia at 33 degrees C combined with sevoflurane (each group n = 7) for 24 hours. The effects on cardiac damage especially on inflammation, apoptosis, and remodeling were studied using cellular and molecular approaches. Five animals were sham operated. Animals treated with hypothermia had lower troponin T levels (p<0.01), reduced infarct size (34+/-7 versus 57+/-12%; p<0.05) and improved left ventricular function compared to normothermia (p<0.05). Hypothermia was associated with a reduction in: (i) immune cell infiltration, (ii) apoptosis, (iii) IL-1beta and IL-6 mRNA up-regulation, and (iv) IL-1beta protein expression (p<0.05). Moreover, decreased matrix metalloproteinase-9 activity was detected in the ischemic myocardium after treatment with mild hypothermia. Sevoflurane conferred additional protective effects although statistic significance was not reached.
Conclusions/significance: Hypothermia reduced myocardial damage and dysfunction after cardiopulmonary resuscitation possible via a reduced rate of apoptosis and pro-inflammatory cytokine expression.
Conflict of interest statement
Figures
References
-
- de Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, van Ree JW, Daemen MJ, et al. Out-of-hospital cardiac arrest in the 1990's: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol. 1997;30:1500–1505. - PubMed
-
- Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106:562–568. - PubMed
-
- Laurent I, Monchi M, Chiche JD, Joly LM, Spaulding C, et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002;40:2110–2116. - PubMed
-
- Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, et al. Post-Cardiac Arrest Syndrome: Epidemiology, Pathophysiology, Treatment, and Prognostication A Consensus Statement From the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–2483. - PubMed
-
- Holzer M, Bernard SA, Hachimi-Idrissi S, Roine RO, Sterz F, et al. Hypothermia for neuroprotection after cardiac arrest: systematic review and individual patient data meta-analysis. Crit Care Med. 2005;33:414–418. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
