

New insights into perinatal testicular torsion
- PMID: 19856186
- PMCID: PMC2859224
- DOI: 10.1007/s00431-009-1096-8
New insights into perinatal testicular torsion
Abstract
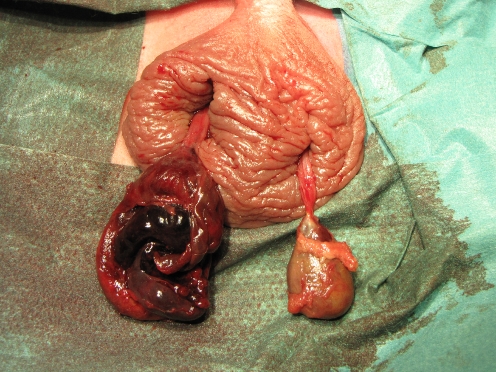
Perinatal testicular torsion is a relatively rare event that remains unrecognized in many patients or is suspected and treated accordingly only after an avoidable loss of time. The authors report their own experience with several patients, some of them quite atypical but instructive. Missed bilateral torsion is an issue, as are partial torsion, possible antenatal signs, and late presentation. These data are discussed together with the existing literature and may help shed new light on the natural course of testicular torsion and its treatment. The most important conclusion is that a much higher index of suspicion based on clinical findings is needed for timely detection of perinatal torsion. It is the authors' opinion that immediate surgery is mandatory not only in suspected bilateral torsions but also in cases of possible unilateral torsions. There is no place for a more fatalistic "wait-and-see" approach. Whenever possible, even necrotic testes should not be removed during surgery because some endocrine function may be retained.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
