

Assessing the burden of pregnancy-associated malaria under changing transmission settings
- PMID: 19863792
- PMCID: PMC2774336
- DOI: 10.1186/1475-2875-8-245
Assessing the burden of pregnancy-associated malaria under changing transmission settings
Abstract
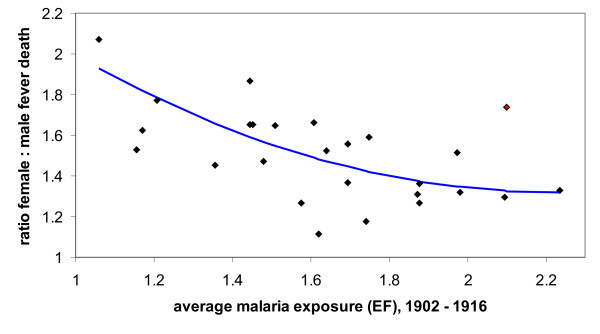
Background: The clinical presentation of pregnancy-associated malaria, or PAM, depends crucially on the particular epidemiological settings. This can potentially lead to an underestimation of its overall burden on the female population, especially in regions prone to epidemic outbreaks and where malaria transmission is generally low.
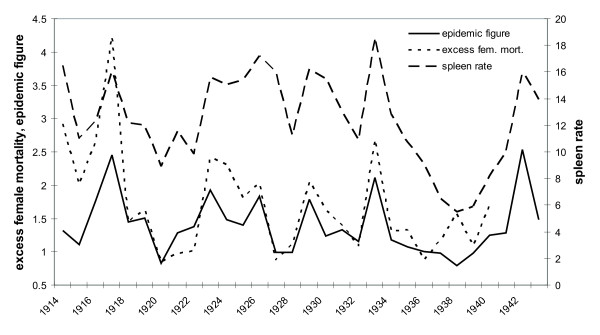
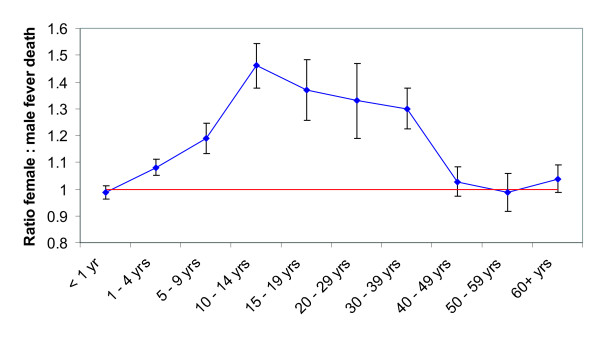
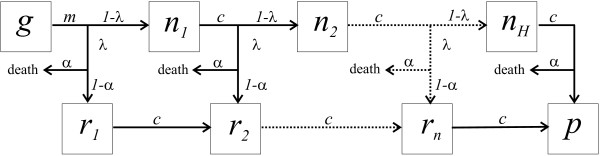
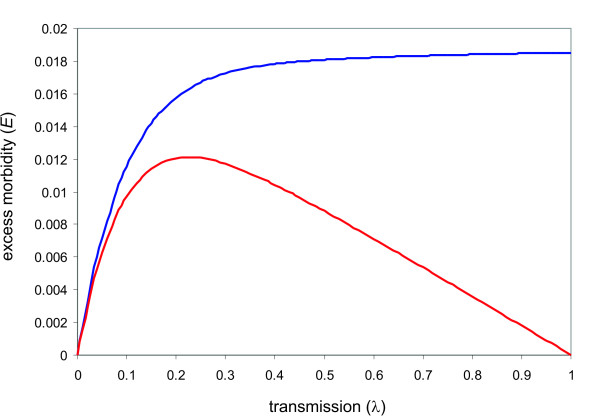
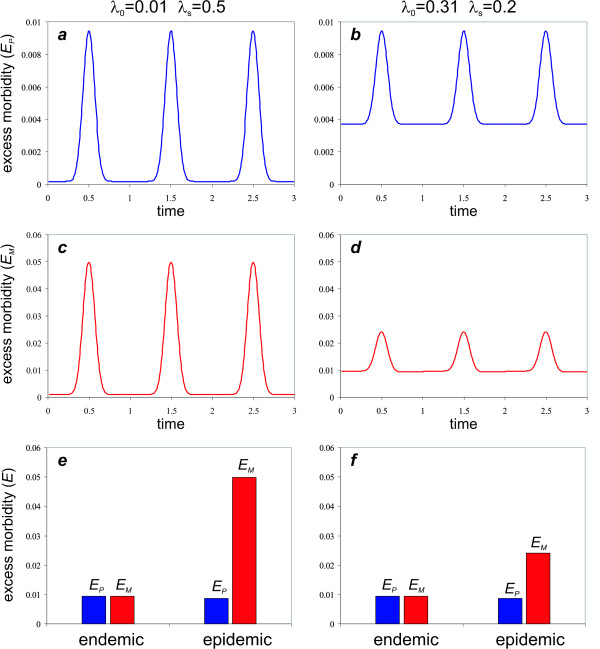
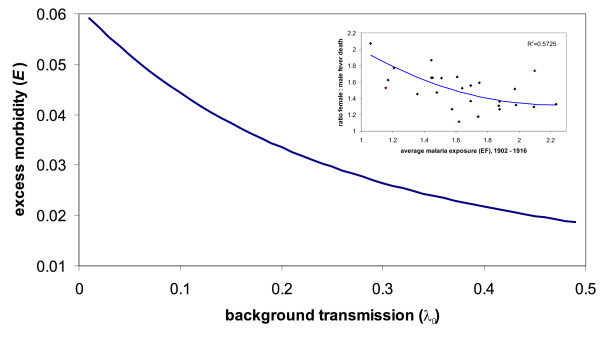
Methods: Here, by re-examining historical data, it is demonstrated how excess female mortality can be used to evaluate the burden of PAM. A simple mathematical model is then developed to highlight the contrasting signatures of PAM within the endemicity spectrum and to show how PAM is influenced by the intensity and stability of transmission.
Results: Both the data and the model show that maternal malaria has a huge impact on the female population. This is particularly pronounced in low-transmission settings during epidemic outbreaks where excess female mortality/morbidity can by far exceed that of a similar endemic setting.
Conclusion: The results presented here call for active intervention measures not only in highly endemic regions but also, or in particular, in areas where malaria transmission is low and seasonal.
Figures
Similar articles
-
Malaria in pregnancy in rural Mozambique: the role of parity, submicroscopic and multiple Plasmodium falciparum infections.Trop Med Int Health. 2002 Jan;7(1):19-28. doi: 10.1046/j.1365-3156.2002.00831.x. Trop Med Int Health. 2002. PMID: 11851951
-
Effectiveness of intermittent preventive treatment with sulfadoxine-pyrimethamine during pregnancy on placental malaria, maternal anaemia and birthweight in areas with high and low malaria transmission intensity in Tanzania.Trop Med Int Health. 2014 Sep;19(9):1048-56. doi: 10.1111/tmi.12349. Epub 2014 Jun 26. Trop Med Int Health. 2014. PMID: 24965022
-
Quantifying malaria endemicity in Ethiopia through combined application of classical methods and enzyme-linked immunosorbent assay: an initial step for countries with low transmission initiating elimination programme.Malar J. 2018 Apr 4;17(1):152. doi: 10.1186/s12936-018-2282-9. Malar J. 2018. PMID: 29618357 Free PMC article.
-
Epidemiology and burden of malaria in pregnancy.Lancet Infect Dis. 2007 Feb;7(2):93-104. doi: 10.1016/S1473-3099(07)70021-X. Lancet Infect Dis. 2007. PMID: 17251080 Review.
-
Malaria in pregnancy and the endemicity spectrum: what can we learn?Trends Parasitol. 2004 Sep;20(9):425-32. doi: 10.1016/j.pt.2004.06.007. Trends Parasitol. 2004. PMID: 15324733 Review.
Cited by
-
High prevalence of dhfr and dhps molecular markers in Plasmodium falciparum in pregnant women of Nchelenge district, Northern Zambia.Malar J. 2015 May 6;14:190. doi: 10.1186/s12936-015-0676-5. Malar J. 2015. PMID: 25943379 Free PMC article.
-
Prospects and Pitfalls of Pregnancy-Associated Malaria Vaccination Based on the Natural Immune Response to Plasmodium falciparum VAR2CSA-Expressing Parasites.Malar Res Treat. 2011;2011:764845. doi: 10.4061/2011/764845. Epub 2012 Jan 18. Malar Res Treat. 2011. PMID: 22363896 Free PMC article.
-
Infections with Plasmodium falciparum during pregnancy affect VAR2CSA DBL-5 domain-specific T cell cytokine responses.Malar J. 2016 Sep 21;15(1):485. doi: 10.1186/s12936-016-1525-x. Malar J. 2016. PMID: 27653505 Free PMC article.
-
Towards a strategy for malaria in pregnancy in Afghanistan: analysis of clinical realities and women's perceptions of malaria and anaemia.Malar J. 2015 Nov 4;14:431. doi: 10.1186/s12936-015-0964-0. Malar J. 2015. PMID: 26537247 Free PMC article.
References
-
- Newman RD, Hailemariam A, Jimma D, Degifie A, Kebede D, Rietveld AE, Nahlen BL, Barnwell JW, Steketee RW, Parise ME. Burden of malaria during pregnancy in areas of stable and unstable transmission in Ethiopia during a nonepidemic year. J Infect Dis. 2003;187:1765–1772. doi: 10.1086/374878. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
