

Variability in interpretive performance at screening mammography and radiologists' characteristics associated with accuracy
- PMID: 19864507
- PMCID: PMC2786197
- DOI: 10.1148/radiol.2533082308
Variability in interpretive performance at screening mammography and radiologists' characteristics associated with accuracy
Abstract
Purpose: To identify radiologists' characteristics associated with interpretive performance in screening mammography.
Materials and methods: The study was approved by institutional review boards of University of Washington (Seattle, Wash) and institutions at seven Breast Cancer Surveillance Consortium sites, informed consent was obtained, and procedures were HIPAA compliant. Radiologists who interpreted mammograms in seven U.S. regions completed a self-administered mailed survey; information on demographics, practice type, and experience in and perceptions of general radiology and breast imaging was collected. Survey data were linked to data on screening mammograms the radiologists interpreted between January 1, 1998, and December 31, 2005, and included patient risk factors, Breast Imaging Reporting and Data System assessment, and follow-up breast cancer data. The survey was returned by 71% (257 of 364) of radiologists; in 56% (205 of 364) of the eligible radiologists, complete data on screening mammograms during the study period were provided; these data were used in the final analysis. An evaluation of whether the radiologists' characteristics were associated with recall rate, false-positive rate, sensitivity, or positive predictive value of recall (PPV(1)) of the screening examinations was performed with logistic regression models that were adjusted for patients' characteristics and radiologist-specific random effects.
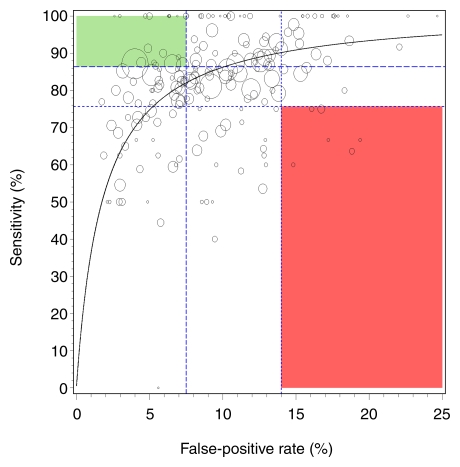
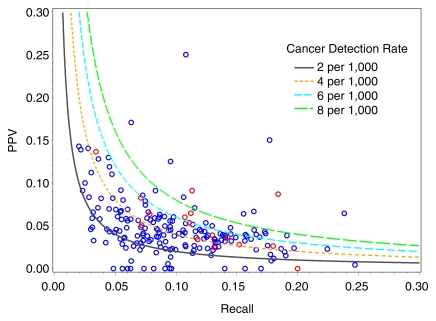
Results: Study radiologists interpreted 1 036 155 screening mammograms; 4961 breast cancers were detected. Median percentages and interquartile ranges, respectively, were as follows: recall rate, 9.3% and 6.3%-13.2%; false-positive rate, 8.9% and 5.9%-12.8%; sensitivity, 83.8% and 74.5%-92.3%; and PPV(1), 4.0% and 2.6%-5.9%. Wide variability in sensitivity was noted, even among radiologists with similar false-positive rates. In adjusted regression models, female radiologists or fellowship-trained radiologists had significantly higher recall and false-positive rates (P < .05, all). Fellowship training in breast imaging was the only characteristic significantly associated with improved sensitivity (odds ratio, 2.32; 95% confidence interval: 1.42, 3.80; P < .001) and the overall accuracy parameter (odds ratio, 1.61; 95% confidence interval: 1.05, 2.45; P = .028).
Conclusion: Fellowship training in breast imaging may lead to improved cancer detection, but it is associated with higher false-positive rates.
Figures
Comment in
-
Mammography: yet another challenge.Radiology. 2009 Dec;253(3):587-9. doi: 10.1148/radiol.2533091517. Radiology. 2009. PMID: 19952020 No abstract available.
References
-
- U.S. Preventive Services Task Force Screening for breast cancer: recommendations and rationale. Ann Intern Med 2002;137(5 pt 1):344–346 - PubMed
-
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 pt 1):347–360 - PubMed
-
- Elmore JG, Wells CK, Lee CH, Howard DH, Feinstein AR. Variability in radiologists’ interpretations of mammograms. N Engl J Med 1994;331(22):1493–1499 - PubMed
-
- Beam CA, Layde PM, Sullivan DC. Variability in the interpretation of screening mammograms by US radiologists: findings from a national sample. Arch Intern Med 1996;156(2):209–213 - PubMed
-
- Smith-Bindman R, Chu P, Miglioretti DL, et al. Physician predictors of mammographic accuracy. J Natl Cancer Inst 2005;97(5):358–367 - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA69976/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- K05 CA104699/CA/NCI NIH HHS/United States
- 1R01 CA107623/CA/NCI NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- R01 CA107623/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- 1K05 CA104699/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
