

The occult pneumothorax: what have we learned?
- PMID: 19865549
- PMCID: PMC2769131
The occult pneumothorax: what have we learned?
Abstract
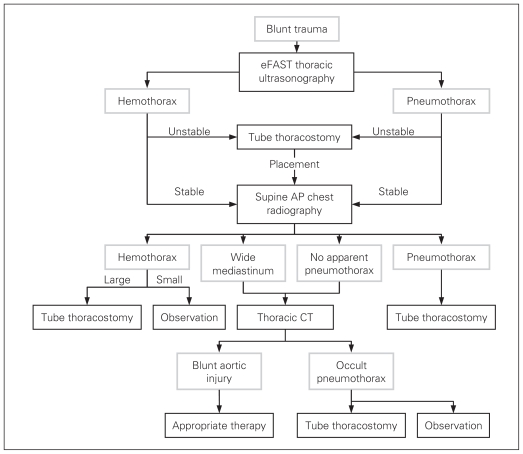
Supine anteroposterior chest radiography is an insensitive test for posttraumatic pneumothoraces. Computed tomography often detects pneumothoraces that were not diagnosed on chest radiography (occult pneumothoraces). Whereas the incidence of occult pneumothoraces approximates 5% of all trauma registry patients, this value approaches 15% among injured patients undergoing computed tomography. Up to 76% of all pneumothoraces may be occult to supine chest radiography with real-time interpretation by trauma teams. Although the size and intrathoracic distribution (anterior) of overt and occult pneumothoraces are similar, significantly more patients with occult pneumothoraces undergo tube thoracostomy compared with those with overt pneumothoraces. This pattern extends both to patients receiving mechanical ventilation and those with penetrating trauma. As an early clinical predictor available during the resuscitation of a trauma patient, only subcutaneous emphysema is predictive of a concurrent occult pneumothorax. The majority of patients with occult pneumothoraces (85%) do not have subcutaneous emphysema, however. Thoracic ultrasonography, as part of a bedside extended focused assessment with sonography for trauma examination, detects 92%-100% of all pneumothoraces and represents a simple extension of the clinician's physical examination. The final remaining question is whether clinicians can safely omit tube thoracostomy in some patients with occult pneumothoraces concurrent to positive pressure ventilation. This omission would avoid subjecting patients to the 22% risk of major chest tube-related insertional, positional and infective complications.
Figures
References
-
- Wall SD, Federle MP, Jeffrey RB, et al. CT diagnosis of unsuspected pneumothorax after blunt abdominal trauma. AJR Am J Roentgenol. 1983;141:919–21. - PubMed
-
- Tocino IM, Miller MH, Frederick PR, et al. CT detection of occult pneumothoraces in head trauma. AJR Am J Roentgenol. 1984;143:987–90. - PubMed
-
- Enderson BL, Abdalla R, Frame SB, et al. Tube thoracostomy for occult pneumothorax: a prospective randomized study of its use. J Trauma. 1993;35:726–30. - PubMed
-
- Brasel KJ, Stafford RE, Weigelt JA, et al. Treatment of occult pneumothoraces from blunt trauma. J Trauma. 1999;46:987–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials