

Intramedullary cavernoma presenting with hematomyelia: report of two girls
- PMID: 19865818
- PMCID: PMC2821515
- DOI: 10.1007/s00381-009-1012-6
Intramedullary cavernoma presenting with hematomyelia: report of two girls
Abstract
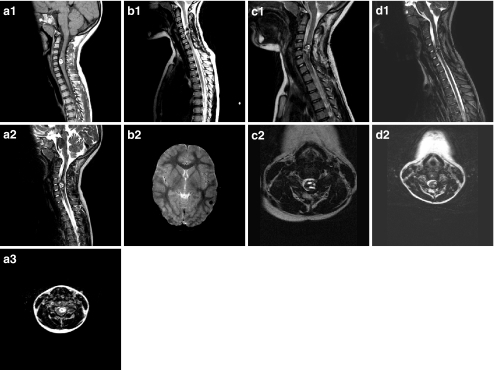
Introduction: Less than 20 children with intramedullary cavernoma (ImC) have been reported in the English literature; however, cases with an unfavorable outcome may be underreported. Whereas these are predominantly boys, we report two girls who presented with hematomyelia (one cervical, one thoracic) and an acute, severe neurological deficit.
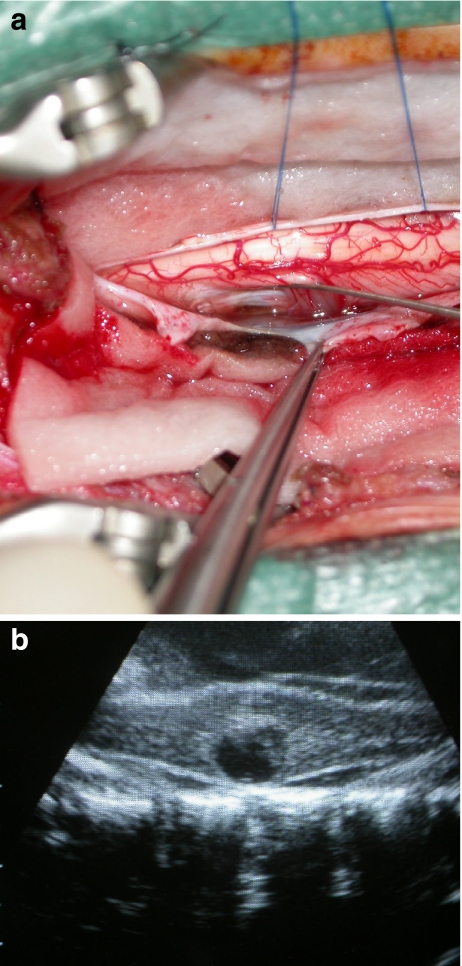
Case material: A 10-year-old girl complaining about lower thoracic pain for several days suddenly developed lower body dysesthesias and paraparesis. Magnetic resonance (MR) demonstrated hematomyelia (T8-T11), intramedullary edema (T6-L1), and an ImC at T9-T10. Within an hour, she progressed to paraplegia and was therefore operated immediately. She slowly recovered regaining independent ambulation and continence. MR after 2 years shows no recurrence. A 7-year-old girl suddenly developed cervicalgia and paresis of her left arm and leg. MR demonstrated hematomyelia and an ImC at C4-C6. She gradually recovered with minimal residual deficit at 3 months and was subsequently operated uneventfully. Multiple cerebral cavernomas and a familial autosomal cavernous malformation syndrome were diagnosed. The following 1.5 years, she complained of intermittent cervicalgia and left brachial dysesthesias, with MR suggesting active residual cavernoma. Interestingly, her complaints gradually disappeared, and she is currently asymptomatic. MR after 3.5 years shows minimal cord swelling no longer suggesting active residual cavernoma.
Conclusion: With adequate surgical treatment either in the acute phase in case of dramatic deterioration or after clinical recuperation, prognosis of symptomatic ImC may be surprisingly good. However, subtotally resected lesions and/or syndromal cases may recur, requiring further treatment. Definitive answers await more cases with longer follow-up.
Figures

References
-
- Craig HD, Gunel M, Cepeda O, Johnson EW, Ptacek L, Steinberg GK, Ogilvy CS, Berg MJ, Crawford SC, Scott RM, Steichen-Gersdorf E, Sabroe R, Kennedy CT, Mettler G, Beis MJ, Fryer A, Awad IA, Lifton RP. Multilocus linkage identifies two new loci for a Mendelian form of stroke, cerebral cavernous malformation, at 7p15–13 and 3q25.2–27. Hum Mol Genet. 1998;7:1851–1858. doi: 10.1093/hmg/7.12.1851. - DOI - PubMed
-
- Deutsch H, Jallo GI, Faktorovich A, Epstein F. Spinal intramedullary cavernoma: clinical presentation and surgical outcome. J Neurosurg. 2000;93:65–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
