

Incidence of propofol-related infusion syndrome in critically ill adults: a prospective, multicenter study
- PMID: 19874582
- PMCID: PMC2784401
- DOI: 10.1186/cc8145
Incidence of propofol-related infusion syndrome in critically ill adults: a prospective, multicenter study
Abstract
Introduction: While propofol is associated with an infusion syndrome (PRIS) that may cause death, the incidence of PRIS is unknown. Determining the incidence of PRIS and the frequency of PRIS-related clinical manifestations are key steps prior to the completion of any controlled studies investigating PRIS. This prospective, multicenter study sought to determine the incidence of PRIS and PRIS-related clinical manifestations in a large cohort of critically ill adults prescribed propofol.
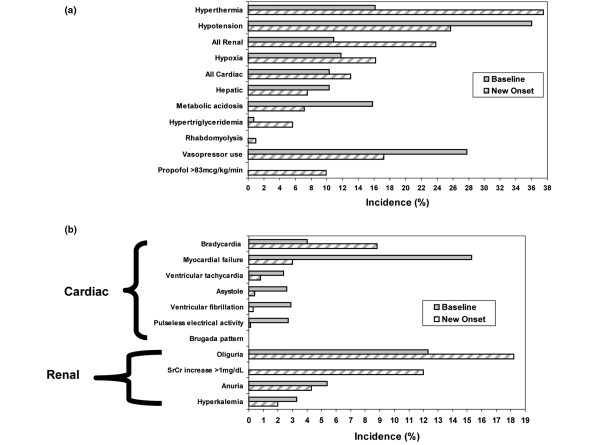
Methods: Critically ill adults from 11 academic medical centers administered an infusion of propofol for [>or=] 24 hours were monitored at baseline and then on a daily basis until propofol was discontinued for the presence of 11 different PRIS-associated clinical manifestations and risk factors derived from 83 published case reports of PRIS.
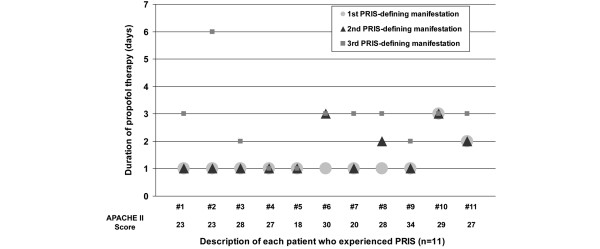
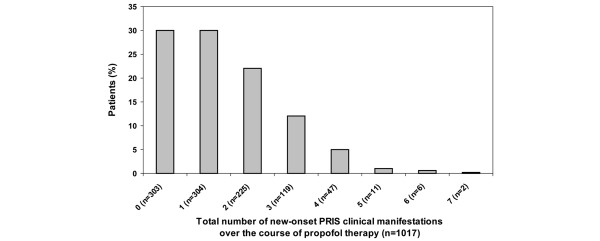
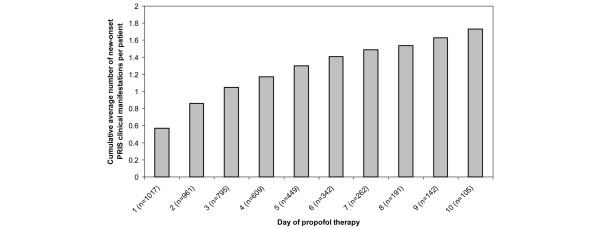
Results: Among 1017 patients [medical (35%), neurosurgical (25%)], PRIS (defined as metabolic acidosis plus cardiac dysfunction and [>or=] 1 of: rhabdomyolysis, hypertriglyceridemia or renal failure occurring after the start of propofol therapy) developed in 11 (1.1%) patients an average of 3 (1-6) [median (range)] days after the start of propofol. While most (91%) of the patients who developed PRIS were receiving a vasopressor (80% initiated after the start of propofol therapy), few received a propofol dose >83 mcg/kg/min (18%) or died (18%). Compared to the 1006 patients who did not develop PRIS, the APACHE II score (25 +/- 6 vs 20 +/- 7, P = 0.01) was greater in patients with PRIS but both the duration of propofol use (P = 0.43) and ICU length of stay (P = 0.82) were similar.
Conclusions: Despite using a conservative definition for PRIS, and only considering new-onset PRIS clinical manifestations, the incidence of PRIS slightly exceeds 1%. Future controlled studies focusing on evaluating whether propofol manifests the derangements of critical illness more frequently than other sedatives will need to be large. These studies should also investigate the mechanism(s) and risk factors for PRIS.
Figures
Comment in
-
The propofol infusion syndrome: more puzzling evidence on a complex and poorly characterized disorder.Crit Care. 2009;13(6):1012. doi: 10.1186/cc8177. Epub 2009 Dec 7. Crit Care. 2009. PMID: 20017894 Free PMC article.
References
-
- Jacobi J, Fraser GL, Coursin DB, Riker RR, Fontaine D, Wittbrodt ET, Chalfin DB, Masica MF, Bjerke HS, Coplin WM, Crippen DW, Fuchs BD, Kelleher RM, Marik PE, Nasraway SA, Murray MJ, Peruzzi WT, Lumb PD. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30:119–141. doi: 10.1097/00003246-200201000-00020. - DOI - PubMed
-
- Abrahams JM, Reiter GT, Acker MA, Sinson GP. Propofol. J Neurosurg. 2002;96:1160–1161. author reply 1161. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
