

A retrospective cohort pilot study to evaluate a triage tool for use in a pandemic
- PMID: 19874595
- PMCID: PMC2784402
- DOI: 10.1186/cc8146
A retrospective cohort pilot study to evaluate a triage tool for use in a pandemic
Abstract
Introduction: The objective of this pilot study was to assess the usability of the draft Ontario triage protocol, to estimate its potential impact on patient outcomes, and ability to increase resource availability based on a retrospective cohort of critically ill patients cared for during a non-pandemic period.
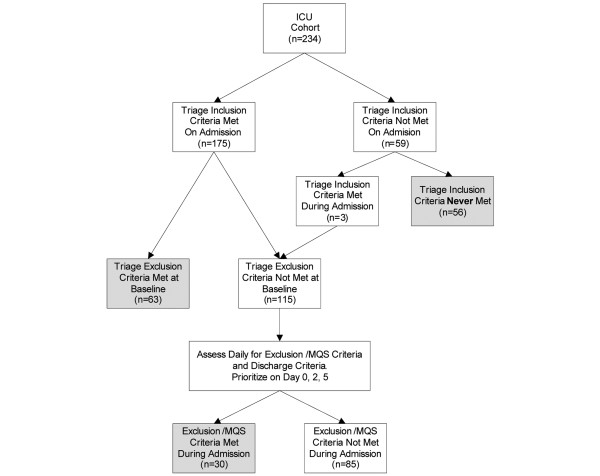
Methods: Triage officers applied the protocol prospectively to 2 retrospective cohorts of patients admitted to 2 academic medical/surgical ICUs during an 8 week period of peak occupancy. Each patient was assigned a treatment priority (red -- 'highest', yellow -- 'intermediate', green -- 'discharge to ward', or blue/black -- 'expectant') by the triage officers at 3 separate time points (at the time of admission to the ICU, 48, and 120 hours post admission).
Results: Overall, triage officers were either confident or very confident in 68.4% of their scores; arbitration was required in 54.9% of cases. Application of the triage protocol would potentially decrease the number of required ventilator days by 49.3% (568 days) and decrease the total ICU days by 52.6% (895 days). On the triage protocol at ICU admission the survival rate in the red (93.7%) and yellow (62.5%) categories were significantly higher then that of the blue category (24.6%) with associated P values of < 0.0001 and 0.0003 respectively. Further, the survival rate of the red group was significantly higher than the overall survival rate of 70.9% observed in the cohort (P < 0.0001). At 48 and 120 hours, survival rates in the blue group increased but remained lower then the red or yellow groups.
Conclusions: Refinement of the triage protocol and implementation is required prior to future study, including improved training of triage officers, and protocol modification to minimize the exclusion from critical care of patients who may in fact benefit. However, our results suggest that the triage protocol can help to direct resources to patients who are most likely to benefit, and help to decrease the demands on critical care resources, thereby making available more resources to treat other critically ill patients.
Figures
Comment in
-
The triage dilemma: opening Pandora's box... ever so slowly.Crit Care. 2010;14(1):401. doi: 10.1186/cc8215. Epub 2010 Jan 19. Crit Care. 2010. PMID: 20092613 Free PMC article. No abstract available.
-
Worst case: rethinking tertiary triage protocols in pandemics and other health emergencies.Crit Care. 2010;14(1):103. doi: 10.1186/cc8216. Epub 2010 Jan 21. Crit Care. 2010. PMID: 20122291 Free PMC article.
References
-
- Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, Ramirez-Venegas A, Rojas-Serrano J, Ormsby CE, Corrales A, Higuera A, Mondragon E, Cordova-Villalobos JA. Pneumonia and Respiratory Failure from Swine-Origin Influenza A (H1N1) in Mexico. N Engl J Med. 2009;361:680–689. doi: 10.1056/NEJMoa0904252. - DOI - PubMed
-
- Christian MD, Devereaux AV, Dichter JR, Geiling JA, Rubinson L. Definitive care for the critically ill during a disaster: current capabilities and limitations: from a Task Force for Mass Critical Care summit meeting, January 26-27, 2007, Chicago, IL. Chest. 2008;133:8S–17S. doi: 10.1378/chest.07-2707. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
