

Implementation of the Canadian C-Spine Rule: prospective 12 centre cluster randomised trial
- PMID: 19875425
- PMCID: PMC2770593
- DOI: 10.1136/bmj.b4146
Implementation of the Canadian C-Spine Rule: prospective 12 centre cluster randomised trial
Abstract
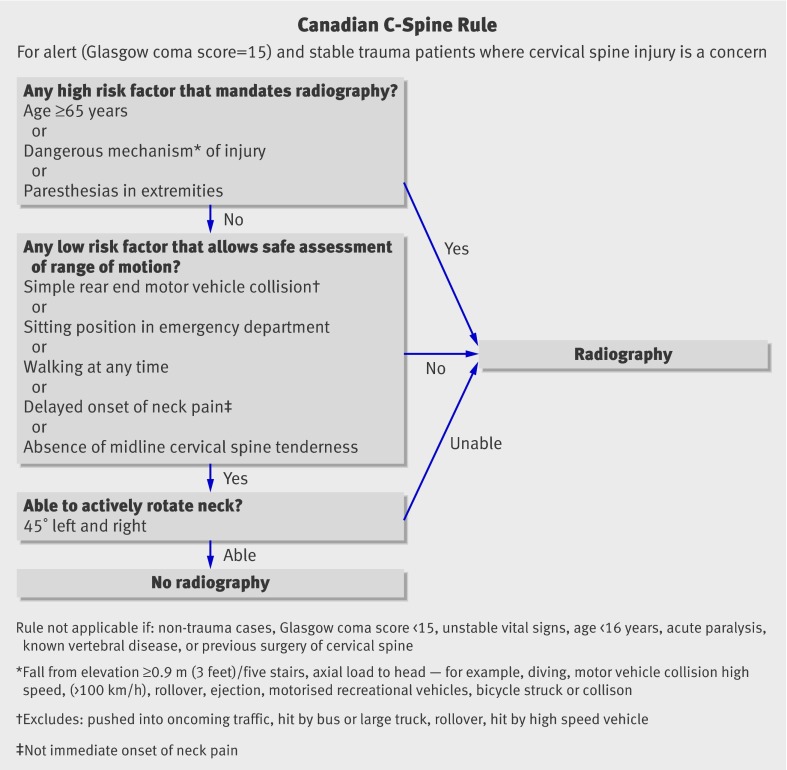
Objective: To evaluate the effectiveness of an active strategy to implement the validated Canadian C-Spine Rule into multiple emergency departments.
Design: Matched pair cluster randomised trial.
Setting: University and community emergency departments in Canada. Participants 11 824 alert and stable adults presenting with blunt trauma to the head or neck at one of 12 hospitals.
Interventions: Six hospitals were randomly allocated to the intervention and six to the control. At the intervention sites, active strategies were used to implement the Canadian C-Spine Rule, including education, policy, and real time reminders on radiology requisitions. No specific intervention was introduced to alter the behaviour of doctors requesting cervical spine imaging at the control sites.
Main outcome measure: Diagnostic imaging rate of the cervical spine during two 12 month before and after periods.
Results: Patients were balanced between control and intervention sites. From the before to the after periods, the intervention group showed a relative reduction in cervical spine imaging of 12.8% (95% confidence interval 9% to 16%; 61.7% v 53.3%; P=0.01) and the control group a relative increase of 12.5% (7% to 18%; 52.8% v 58.9%; P=0.03). These changes were significant when both groups were compared (P<0.001). No fractures were missed and no adverse outcomes occurred.
Conclusions: Implementation of the Canadian C-Spine Rule led to a significant decrease in imaging without injuries being missed or patient morbidity. Final imaging rates were much lower at intervention sites than at most US hospitals. Widespread implementation of this rule could lead to reduced healthcare costs and more efficient patient flow in busy emergency departments worldwide.
Trial registration: Clinical trials NCT00290875.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Prediction rules in cervical spine injury.BMJ. 2009 Oct 29;339:b4139. doi: 10.1136/bmj.b4139. BMJ. 2009. PMID: 19875424 No abstract available.
-
The Canadian C-spine rule safely reduces imaging rates for cervical spine injuries.J Physiother. 2010;56(1):59. doi: 10.1016/s1836-9553(10)70057-6. J Physiother. 2010. PMID: 20500140 No abstract available.
References
-
- McCaig LF, Nawar EW. National hospital ambulatory medical care survey: 2004 Emergency department summary. Adv Data 2006;372. - PubMed
-
- Hoffman JR, Mower W, Wolfson AB, Todd K, Zucker M. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. N Engl J Med 2000;343:94-9. - PubMed
-
- Martin DR, Semelka RC. Health effects of ionising radiation from diagnostic CT. Lancet 2006;367:1712-4. - PubMed
-
- Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med 2007;357:2277-84. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical