

The liver transplant waiting list--a single-center analysis
- PMID: 1987681
- PMCID: PMC3091381
- DOI: 10.1097/00007890-199101000-00020
The liver transplant waiting list--a single-center analysis
Abstract
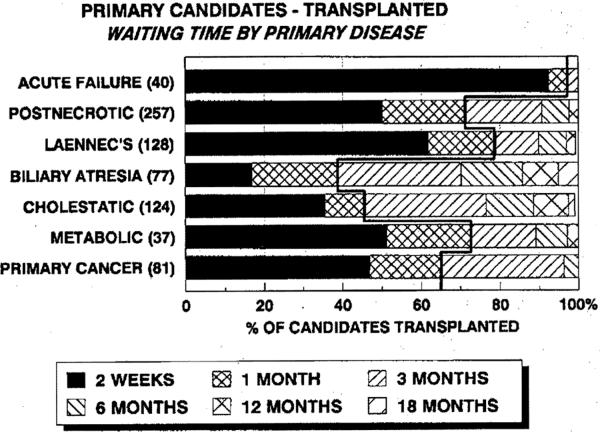
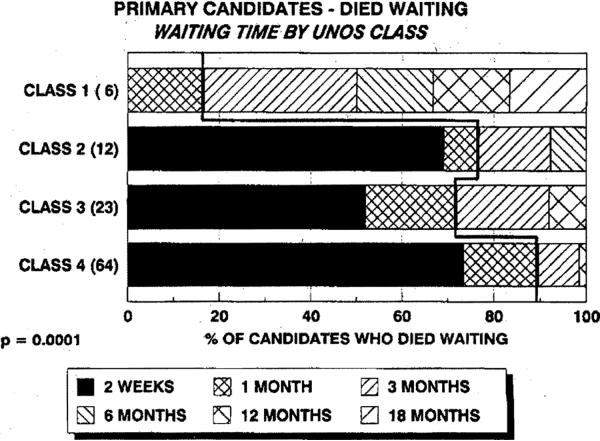
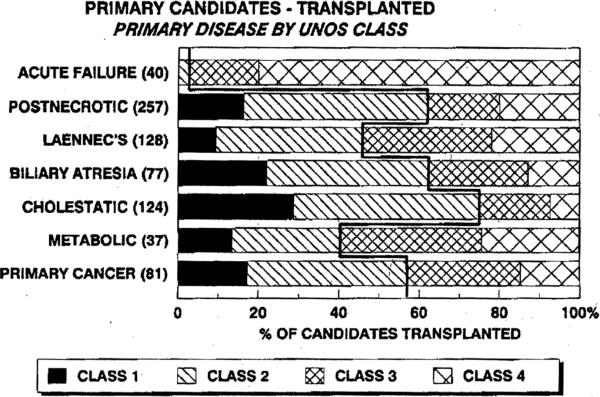
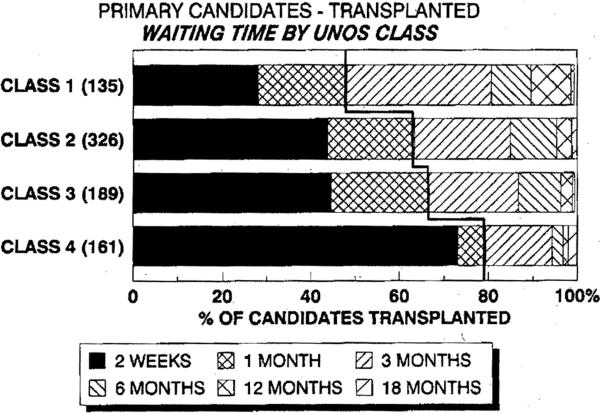
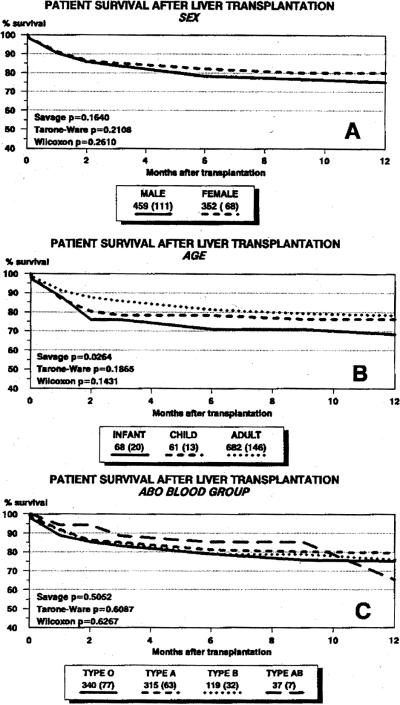
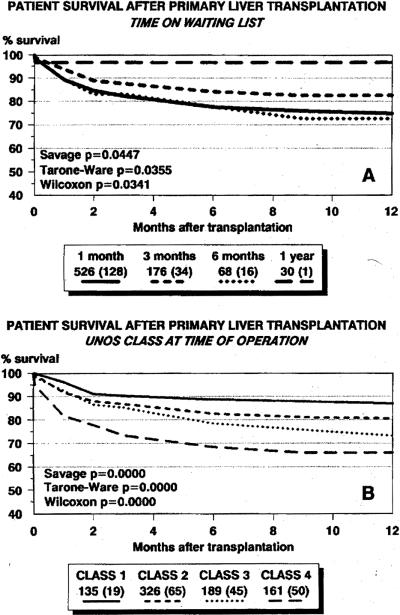
At this transplant center 1340 patients were entered on the liver transplant waiting list during the first 25 months (October 1987 to November 1989) after the initiation of the UNOS allocation system for liver grafts. Of these 972 (72.5%) of the patients received a graft, 120 (9.0%) died waiting for a graft, 109 (8.1%) remained on the active list as of the study endpoint of December 15, 1989, 123 (9.2%) were withdrawn from candidacy, and 16 (1.2%) received a transplant at another center. A total of 1201 patients were candidates for a first graft. Of the 812 primary candidates who received a graft, 64.8% received their graft within one month of entry on the waiting list. Of the 109 primary candidates who died before a graft could be found, 79.0% died within a month of entry onto the waiting list. At time of transplantation, 135 (16.6%) primary recipients of a graft were UNOS class 1, 326 (40.1%) were UNOS class 2, 190 (23.4%) were UNOS class 3, and 161 (19.8%) were UNOS class 4. Actuarial survival rates (percentage) at 6 months for recipients in UNOS class 1, class 2, class 3, and class 4 were 88.7 +/- 2.9, 82.6 +/- 2.1, 78.4 +/- 3.2, and 68.4 +/- 3.9, respectively (P less than 0.001). At the time of death of recipients who failed to get a graft, 6 (5.5%) were UNOS class 1, 14 (12.8%) were UNOS class 2, 23 (21.1%) were UNOS class 3, and 66 (60.6%) were UNOS class 4. These results indicate that a high proportion of liver transplant candidates are in urgent need of a graft and that the UNOS system succeeds in giving these patients high priority. However patient mortality on the waiting list and after transplantation would lessen significantly if more patients with end-stage liver disease were referred to the transplant center in a timely manner before their condition reaches the point where the probability of survival is diminished.
Figures
References
-
- Shaw BW, Jr, Wood RP, Stratta RJ, et al. Stratifying the causes of death in liver transplant recipients: an approach to improving survival. Arch Surg. 1989;124:895. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical