

Congenital Trypanosoma cruzi transmission in Santa Cruz, Bolivia
- PMID: 19877966
- PMCID: PMC5454522
- DOI: 10.1086/648070
Congenital Trypanosoma cruzi transmission in Santa Cruz, Bolivia
Abstract
Background: We conducted a study of congenital Trypanosoma cruzi infection in Santa Cruz, Bolivia. Our objective was to apply new tools to identify weak points in current screening algorithms, and find ways to improve them.
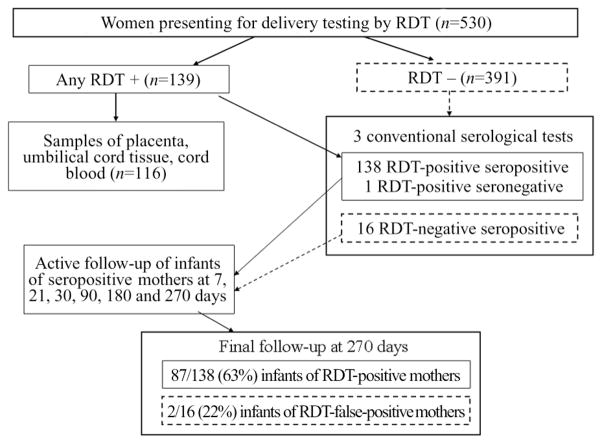
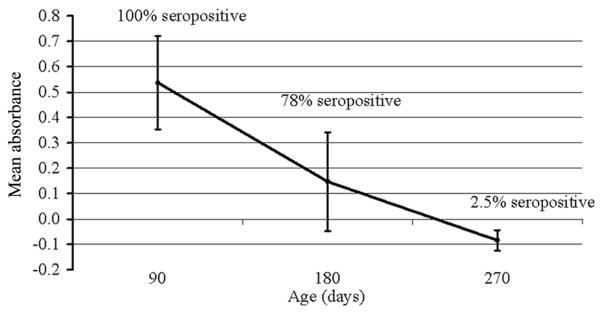
Methods: Women presenting for delivery were screened by rapid and conventional serological tests. For infants of infected mothers, blood specimens obtained on days 0, 7, 21, 30, 90, 180, and 270 were concentrated and examined microscopically; serological tests were performed for the day 90, 180, and 270 specimens. Maternal and infant specimens, including umbilical tissue, were tested by polymerase chain reaction (PCR) targeting the kinetoplast minicircle and by quantitative PCR.
Results: Of 530 women, 154 (29%) were seropositive. Ten infants had congenital T. cruzi infection. Only 4 infants had positive results of microscopy evaluation in the first month, and none had positive cord blood microscopy results. PCR results were positive for 6 (67%) of 9 cord blood and 7 (87.5%) of 8 umbilical tissue specimens. PCR-positive women were more likely to transmit T. cruzi than were seropositive women with negative PCR results (P < .05). Parasite loads determined by quantitative PCR were higher for mothers of infected infants than for seropositive mothers of uninfected infants P < .01). Despite intensive efforts, only 58% of at-risk infants had a month 9 specimen collected.
Conclusions: On the basis of the low sensitivity of microscopy in cord blood and high rate of loss to follow-up, we estimate that current screening programs miss one-half of all infected infants. Molecular techniques may improve early detection.
Figures
Comment in
-
New advances in the management of a long-neglected disease.Clin Infect Dis. 2009 Dec 1;49(11):1685-7. doi: 10.1086/648073. Clin Infect Dis. 2009. PMID: 19877968 No abstract available.
References
-
- Dias JC, Silveira AC, Schofield CJ. The impact of Chagas disease control in Latin America: a review. Mem Inst Oswaldo Cruz. 2002;97:603–12. - PubMed
-
- Organización Panamericana de la Salud. Estimación cuantitativa de la enfermedad de Chagas en las Americas. Montevideo, Uruguay: Organización Panamericana de la Salud; 2006.
-
- Schenone H, Gaggero M, Sapunar J, Contreras MC, Rojas A. Congenital Chagas disease of second generation in Santiago, Chile: report of two cases. Rev Inst Med Trop Sao Paulo. 2001;43:231–2. - PubMed
-
- Azogue E, Darras C. Prospective study of Chagas disease in newborn children with placental infection caused by Trypanosoma cruzi (Santa Cruz-Bolivia) Rev Soc Bras Med Trop. 1991;24:105–9. - PubMed
-
- Basombrio MA, Nasser J, Segura MA, et al. The transmission de Chagas disease in Salta and the detection of congenital cases. Medicina (B Aires) 1999;59(Suppl 2):143–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
