

Contemporary management of vascular complications associated with Ehlers-Danlos syndrome
- PMID: 19879095
- PMCID: PMC6042287
- DOI: 10.1016/j.jvs.2009.08.019
Contemporary management of vascular complications associated with Ehlers-Danlos syndrome
Abstract
Objectives: There has been debate regarding the safety of performing elective procedures in patients with vascular manifestations associated with Ehlers-Danlos syndrome (EDS). The purpose of this study was to review the surgical management and clinical outcomes of EDS patients undergoing vascular procedures at a tertiary medical center with multimodality expertise in connective tissue disorders.
Methods: All patients with EDS undergoing endovascular and open vascular procedures at a single-institution academic medical center from 1994 to 2009 were retrospectively reviewed. Clinical data were evaluated including patient demographics, length of stay (LOS), and mortality outcomes during hospital course and long-term follow-up.
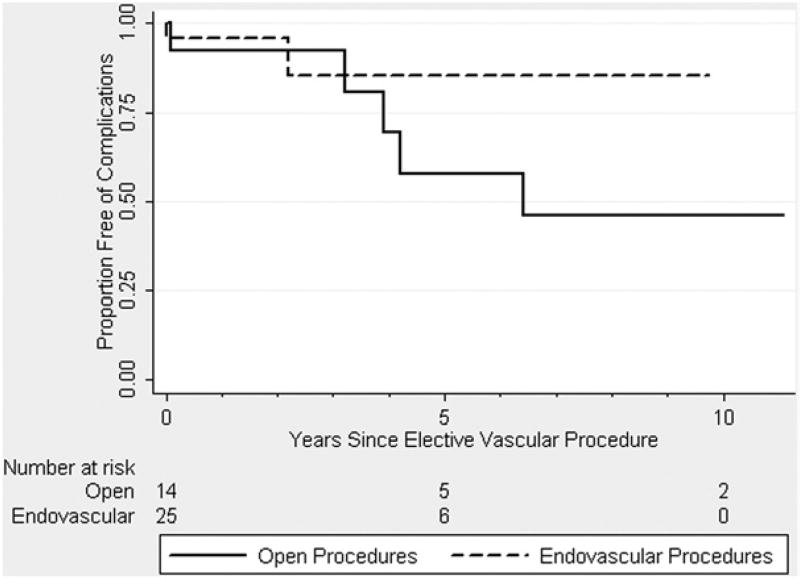
Results: A total of 40 patients with EDS were identified, including individuals diagnosed with classic (n = 15), hypermobility (n = 16), and vascular (n = 9) types of EDS. These patients collectively underwent 45 endovascular and 18 open procedures for vascular disease during the time period, including embolization (n = 37), angioplasty (n = 8), arterial bypass (n = 5), and aortic aneurysm repair (n = 13). All cases were performed electively, except for one (2%) urgent endovascular and one (5%) emergent open procedure. Endovascular procedures were associated with a median LOS (interquartile range [IQR]) of 2 (1 to 3) days with no procedure-related mortality or in-hospital deaths among all EDS types, whereas open vascular procedures had median LOS (IQR) of 6 (5 to 8) days with one (6%) in-hospital death occurring in a vascular EDS patient. Survival free of any complication at 5 years was 85% and 54% following endovascular and open procedures, respectively.
Conclusions: The elective surgical management of vascular disorders in EDS patients using open and endovascular procedures has been associated with good outcomes. Our results suggest that vascular interventions in these EDS patients can be safely performed and should not be withheld until rupture or acute symptoms arise.
Copyright 2010 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a competition of interest.
Figures
References
-
- Steinman B, Royce PM. Superti-Furga: Ehlers-Danlos Syndrome. In: Royce P, Steinmann B, editors. Connective tissue and its heritable disorders. 5. New York: Wiley-Liss; 2002. pp. 431–523.
-
- Byers PH. Ehlers-Danlos Syndrome. In: Rimoin DL, Connor JM, Pyereitz RE, editors. Emery and Rimoin’s principles and practice of medical genetics. 3. London: Churchill Livingstone; 1997. pp. 1067–81.
-
- Cikrit DF, Miles JH, Silver D. Spotaneous arterial perforation: the Ehlers-Danlos specter. J Vasc Surg. 1987;5:248–55. - PubMed
-
- Bergqvist D. Ehlers-Danlos type IV syndrome: a review from a vascular surgical point of view. Eur J Surg. 1996;162:163–70. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
