

Improvement in health-related quality of life after hospitalization predicts event-free survival in patients with advanced heart failure
- PMID: 19879462
- PMCID: PMC2772831
- DOI: 10.1016/j.cardfail.2009.05.003
Improvement in health-related quality of life after hospitalization predicts event-free survival in patients with advanced heart failure
Abstract
Background: Health-related quality of life (HRQOL) is a major clinical outcome for heart failure (HF) patients. We aimed to determine the frequency, durability, and prognostic significance of improved HRQOL after hospitalization for decompensated HF.
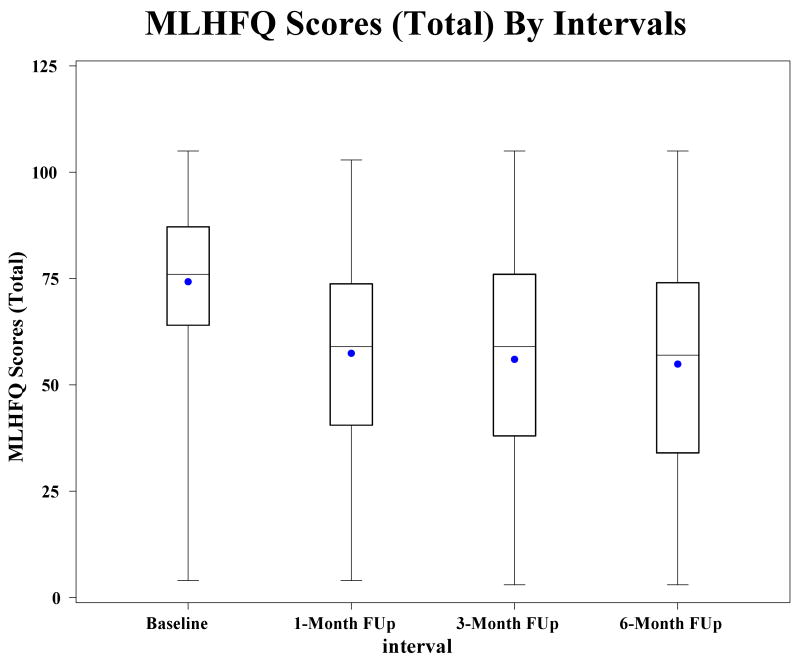
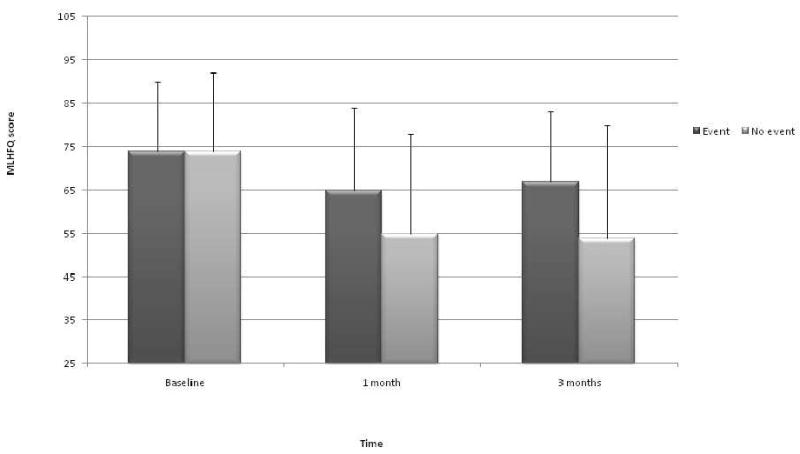
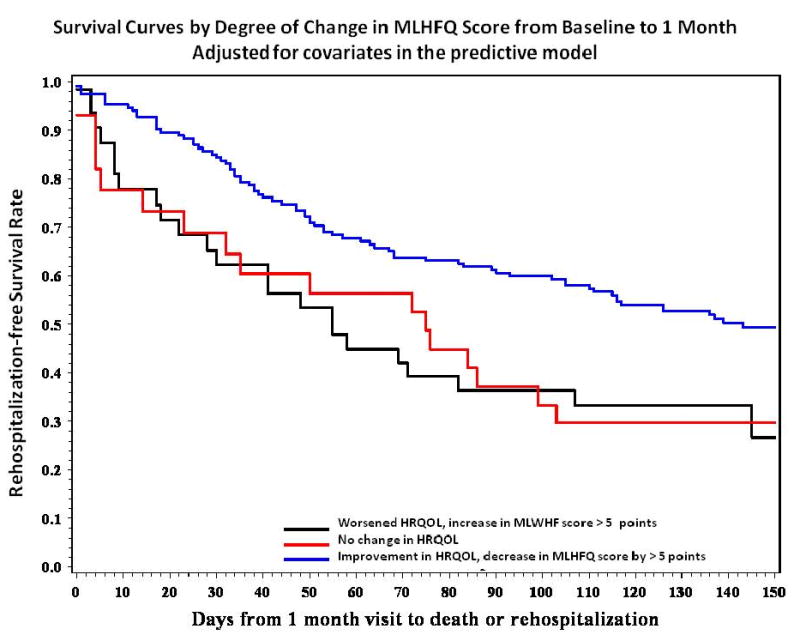
Methods and results: We analyzed HRQOL, measured serially using the Minnesota Living with Heart Failure Questionnaire (MLHFQ), for 425 patients who survived to discharge in a multicenter randomized clinical trial of pulmonary artery catheter versus clinical assessment to guide therapy for patients with advanced HF. All patients enrolled had 1 or more prior HF hospitalizations or chronic high diuretic doses and 1 or more symptom and 1 sign of fluid overload at admission. Improvement, defined as a decrease of more than 5 points in MLHFQ total score, occurred in 68% of patients by 1 month and stabilized. The degree of 1-month improvement differed (P < .0001 group x time interaction) between 6-month survivors and non-survivors. In a Cox regression model, after adjustment for traditional risk factors for HF morbidity and mortality, improvement in HRQOL by 1 month compared to worsening at 1 month or no change predicted time to subsequent event-free survival (P=.013).
Conclusions: In patients hospitalized with severe HF decompensation, HRQOL is seriously impaired but improves substantially within 1 month for most patients and remains improved for 6 months. Patients for whom HRQOL does not improve by 1 month after hospital admission merit specific attention both to improve HRQOL and to address high risk for poor event-free survival.
Conflict of interest statement
Figures
Similar articles
-
Comparison of the Kansas City Cardiomyopathy Questionnaire and Minnesota Living With Heart Failure Questionnaire in Predicting Heart Failure Outcomes.Am J Cardiol. 2019 Mar 1;123(5):807-812. doi: 10.1016/j.amjcard.2018.11.037. Epub 2018 Dec 4. Am J Cardiol. 2019. PMID: 30587373 Free PMC article.
-
Quality of life predicts outcome in a heart failure disease management program.Int J Cardiol. 2010 Feb 18;139(1):60-7. doi: 10.1016/j.ijcard.2008.09.003. Epub 2008 Oct 12. Int J Cardiol. 2010. PMID: 18851887
-
Prognostic value of health-related quality of life in elderly patients hospitalized with heart failure.Clin Interv Aging. 2019 May 22;14:935-945. doi: 10.2147/CIA.S201403. eCollection 2019. Clin Interv Aging. 2019. PMID: 31190779 Free PMC article.
-
Exercise-based cardiac rehabilitation for chronic heart failure: the EXTRAMATCH II individual participant data meta-analysis.Health Technol Assess. 2019 May;23(25):1-98. doi: 10.3310/hta23250. Health Technol Assess. 2019. PMID: 31140973 Free PMC article. Review.
-
Exercise-based cardiac rehabilitation for adults with heart failure.Cochrane Database Syst Rev. 2019 Jan 29;1(1):CD003331. doi: 10.1002/14651858.CD003331.pub5. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2024 Mar 7;3:CD003331. doi: 10.1002/14651858.CD003331.pub6. PMID: 30695817 Free PMC article. Updated.
Cited by
-
Health-Related Quality of Life, Functional Status, and Cardiac Event-Free Survival in Patients With Heart Failure.J Cardiovasc Nurs. 2016 May-Jun;31(3):236-44. doi: 10.1097/JCN.0000000000000248. J Cardiovasc Nurs. 2016. PMID: 25774841 Free PMC article.
-
A Patient-Centered Mobile Phone App (iHeartU) With a Virtual Human Assistant for Self-Management of Heart Failure: Protocol for a Usability Assessment Study.JMIR Res Protoc. 2019 May 23;8(5):e13502. doi: 10.2196/13502. JMIR Res Protoc. 2019. PMID: 31124472 Free PMC article.
-
Psychometric properties of the Symptom Status Questionnaire-Heart Failure.J Cardiovasc Nurs. 2015 Mar-Apr;30(2):136-44. doi: 10.1097/JCN.0000000000000102. J Cardiovasc Nurs. 2015. PMID: 24598550 Free PMC article.
-
Impact of Psoriasis on Quality of Life: Relationship between Clinical Response to Therapy and Change in Health-related Quality of Life.Ann Dermatol. 2010 Nov;22(4):389-96. doi: 10.5021/ad.2010.22.4.389. Epub 2010 Nov 5. Ann Dermatol. 2010. PMID: 21165207 Free PMC article.
-
Hemoglobin A1c improvements and better diabetes-specific quality of life among participants completing diabetes self-management programs: a nested cohort study.Health Qual Life Outcomes. 2012 May 14;10:48. doi: 10.1186/1477-7525-10-48. Health Qual Life Outcomes. 2012. PMID: 22583609 Free PMC article.
References
-
- Sullivan M. The new subjective medicine: taking the patient's point of view on health care and health. Soc Sci Med. 2003;56:1595–1604. - PubMed
-
- Kaplan RM. The significance of quality of life in health care. Qual Life Res. 2003;12:3–16. - PubMed
-
- Stanek EJ, Oates MB, McGhan WF, Denofrio D, Loh E. Preferences for treatment outcomes in patients with heart failure: symptoms versus survival. J Card Fail. 2000;6:225–232. - PubMed
-
- Moser DK, Doering LV, Chung ML. Vulnerabilities of patients recovering from an exacerbation of chronic heart failure. Am Heart J. 2005;150:984. - PubMed
-
- Evangelista LS, Dracup K, Moser DK, Westlake C, Erickson V, Hamilton MA, Fonarow GC. Two-year follow-up of quality of life in patients referred for heart transplant. Heart Lung. 2005;34:187–193. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
